
Robert Koch – Photo gallery

1 (of 2) Robert Koch (third from right) on a German medical expedition to Egypt to study the cholera epidemic, 1884.
Photographer unknown. Public domain, via Wikimedia Commons. Source: KRUIF, Paul de. Mikrobenjäger. Orell Füssli, Zürich, 1927.

2 (of 2) Robert Koch working in his laboratory at Kimberley, South Africa. Photogravure of gouache painting.
Wellcome Images, CC BY 4.0, via Wikimedia Commons
Robert Koch – Nominations
Robert Koch – Facts
Robert Koch – Other resources
Links to other sites
On Robert Koch from Harvard University Library
On Robert Koch from Robert Koch Institut
Robert Koch – Nobel Lecture
Nobel Lecture, December 12, 1905
The Current State of the Struggle against Tuberculosis
Twenty years ago, tuberculosis, even in its most dangerous form, consumption, was still not considered infectious. Of course, the work of Villemin and the experimental investigations by Cohnheim and Salomonsen had already provided certain clues which suggested that this conception was false. But it was only with the discovery of the tubercle bacillus that the aetiology of tuberculosis was placed on a firm footing, and the conviction gained that this is a parasitic disease, i.e. an infectious, but also avoidable one.
In the first papers concerning the aetiology of tuberculosis I have already indicated the dangers arising from the spread of the bacilli-containing excretions of consumptives, and have urged moreover that prophylactic measures should be taken against the contagious disease. But my words have been un-heeded. It was still too early, and because of this they still could not meet with full understanding. It shared the fate of so many similar cases in medicine, where a long time has also been necessary before old prejudices were overcome and the new facts were acknowledged to be correct by the physicians.
However, quite gradually the understanding of the infectious nature of tuberculosis then spread, taking root ever more deeply, and the more the conviction of the dangerous nature of tuberculosis made headway, the more was the necessity of protecting oneself against it thrust on people.
First of all, efforts directed to this end attracted attention in papers giving information and warnings. Shortly after this there came into existence, provoked by the successes which Brehmer obtained with the dietetic-hygienic treatment of patients with lung complaints, sanatoria for consumptives, to which were added convalescent homes, seaside resorts, out-patient clinics and similar establishments. An extremely rich corporate activity developed. International congresses took place. In some places the obligation to give notice to the authorities was introduced, on an optional or compulsory basis. In some states and cities thoroughly worked-out laws were enacted against the tuberculosis menace. Hardly a country remains where, in one way or another, the struggle against tuberculosis has not been taken up, and it is extraordinarily gratifying to see how the campaign is now waged quite generally and with considerable vigour against this dangerous enemy.
But taken as a whole, all these efforts were quite dissimilar in character, though they all pursued the same aim, but chose quite different approaches to it. In one country people wanted to achieve everything by instruction, in another they hoped to be able to remove tuberculosis by therapeutic measures, and again in another people turned exclusively against the supposed menacing dangers of bovine tuberculosis. Of late a certain adjustment has, indeed, made its appearance, in so far as individual countries no longer proceed in quite such a biased way as before, and one takes over from another whatever seems to be well tried in the way of means of defense. However, amidst the persistently great variety in the ways and means of combating tuberculosis, it is yet necessary to ask what measures do indeed best satisfy the scientific requirements and general findings in the fight against contagious disease.
But, before we come to answer this question, we must make perfectly clear to ourselves how infection is brought about in tuberculosis, i.e. how the tubercle bacilli invade the human organism; for all prophylactic measures against an infectious disease can only be directed towards preventing the germs of disease from invading the body.
In relation to tuberculosis infection so far only two possibilities have offered themselves: first, infection by tubercle bacilli which come from tuberculous people, and second, by those that are contained in the milk and meat of tuberculous cattle.
As a result of investigations which I made together with Schütz into the relation between human and bovine tuberculosis, we can dismiss this second possibility, or look upon it as being so small that this source of infection is quite overshadowed by the other. We arrived in effect at the conclusion that human and bovine tuberculosis are different from one another, and that bovine tuberculosis cannot be transmitted to a human. With regard to this latter point, I would, however, like to add, so as to obviate misunderstandings, that I refer only to those forms of tuberculosis which are of some account in the fight against tuberculosis as an epidemic, namely to generalized tuberculosis, and, above all, to consumption. It would take us too far here, if I were to go more closely into the very lively discussion which has developed over this question; I must keep this for some other occasion. I would just like to observe in addition to this that the re-examination of our investigations, which was undertaken in the Imperial Department of Health in Berlin with the greatest care and over a wide area, has led to a confirmation of my view, and that the harmlessness for humans of the bacilli of “pearl disease” is directly proved, in addition, by inoculating humans with material from it, as was done by Spengler and Klemperer. Consequently, only the tubercle bacilli coming from humans are of consequence in the battle against tuberculosis.
But the disease does not in all tuberculous patients take such forms that tubercle bacilli are discharged to a noteworthy extent. It is really only those suffering from tuberculosis of the larynx and lungs who produce and disseminate considerable quantities of tubercle bacilli in a dangerous way. But it is as well to note that not only is the secretion of the lung called sputum dangerous by reason of its bacillary content, but that, according to the investigations of Flügge, even the smallest drops of mucus expelled into the air by the patient when he coughs, clears his throat, and even speaks, contain bacilli and can cause infection.
We come therefore to this fairly sharp demarcation, that only those tuberculous patients comprise an important danger to the people around them, who suffer from laryngeal or pulmonary tuberculosis and have sputum which contains bacilli. This type of tuberculosis is designated “open” as opposed to “closed”, in which no tubercle bacilli are discharged into the environment.
But even in patients with open tuberculosis there are still distinctions to be made regarding the degree of danger due to them.
It can indeed very often be observed that such patients live for years with their families, without infecting any of them. Under some circumstances, in hospitals for consumptives infections among the nursing staff can be totally absent, or indeed so rare that it was even thought that in this was to be seen a proof of the non-contagiousness of tuberculosis. If, however, such cases are looked into more thoroughly, then it turns out that there are good reasons for the apparent lack of contagiousness. In such cases one is dealing with patients who are very careful where their sputum is concerned, who value the cleanliness of their home and their clothing, and in addition live in well-aired and well-lit rooms, so that the germs, taken up in air, can be rapidly carried away by the flow of air or killed by light. If these conditions are not fulfilled, then infection is not lacking in hospitals and the homes of the well-to-do, as experience teaches us every day. It becomes more frequent, the more unhygienically the patients handle their expectoration, the more there is a lack of light and air, and the more closely the sick are crowded together with the healthy. The risk of infection becomes particularly high if healthy people have to sleep with the sick in the same rooms, and especially, as still unfortunately happens with the poorer section of the population, in one and the same bed.
In the eyes of careful observers, this sort of infection has acquired such importance that tuberculosis has been called plainly, and quite justly, a disease of accommodation.
To recapitulate briefly, the circumstances relating to infection in tuberculosis are as follows.
Patients with closed tuberculosis are to be regarded as quite harmless. Also people suffering from open tuberculosis are harmless as long as the tubercle bacilli discharged by them are prevented from causing infection by cleanliness, ventilation, etc. The patient only becomes dangerous, when he is on his own unclean, or when, as the result of advanced disease, he becomes so helpless that he can no longer see to the adequate disposal of the expectorated material. At the same time the risk of the healthy being infected increases with the impossibility of avoiding the immediate neighbourhood of the dangerous patient, thus in crowded rooms and most particularly when these are not only overfull, but are badly ventilated and inadequately illuminated as well.
I now come to the problem of examining the measures currently in use to see to what extent they take account of the aetiological factors, as I have just described them. If I prefer to confine myself in this to the conditions in Germany, this is because these are the ones I know best, and because it would not be possible to carry out a survey of the factors in other countries in a single lecture.
The starting-point in the fight against all contagious diseases is the obligation to report, because without this most cases of the disease remain unknown. So we must make this a requirement for tuberculosis as well. But in this particular disease, out of consideration towards the patients, there has been some reluctance to require the notification to be given by the doctors or those otherwise under an obligation to do so. However with the correct realization that it is not just a question of considerations applying to the sick here but also of the protection of the healthy, the obligation to notify has been introduced in several places, at first on an optional basis, and then, when it transpired that the disadvantages feared did not materialize, on a compulsory basis. Since, therefore, experience has already testified to the feasibility of registration in tuberculosis, it should be introduced everywhere. It can, however, without prejudicing the objective, be restricted to those cases which constitute a danger to their acquaintances and so to patients with open tuberculosis in hygienically unfavourable conditions.
If we lay the responsibility for notification on doctors, then we must at the same time ensure that they can judge the cases in question correctly, in particular with respect to the presence of open tuberculosis. This can only happen with the establishment of centres where the patient’s sputum is examined without cost for tubercle bacilli. These could exist independently, or, what is perhaps more practical, in association with hospitals, policlinics, or with social-welfare centres, which will be mentioned later. So far such places for investigations have already been established in some countries, but in far too small numbers. It will be necessary in future to take this need into consideration adequately.
Now what is to happen to the patients who are to be regarded as dangerous, after they have been identified?
If it would be possible to place all these people together in hospitals and thus make them relatively harmless, then tuberculosis would decrease very rapidly.
But this, for the moment at least, is out of the question. The number of people with tuberculosis for whom hospital treatment would be necessary is in Germany, for example, estimated at more than 200,000. To place so many patients in institutions would require enormous funds.
However, it is by no means necessary that all tuberculous patients should be brought into hospitals at once. We may count on a decrease in tuberculosis, albeit a slower one, if a considerable fraction of these patients are admitted into suitable institutions.
In connection with this, let me remind you of the exceptionally instructive example of the fight against leprosy in Norway. Not all lepers were isolated in that country either, but only a fraction of them, among which, however, were just those who were especially dangerous; in this way they have obtained the result that the number of lepers, which amounted to nearly 3,000 in 1856, has declined to about 500 at the present time.
One should proceed in the fight against tuberculosis along the lines suggested by this example. And, if it is not possible to deal with all consumptives, then as many as is humanly possible, including the most dangerous, i.e. those who are in the final stages of consumption, should be accommodated in hospitals.
In this respect, however, already there is more happening in some places than is usually supposed. In the city of Berlin over the last decade more than 40% of consumptives have died in hospitals. The circumstances must be fairly favourable in Stockholm as well, since Carlsson states in his paper on the fight against tuberculosis in Sweden that 410 consumptives were cared for in the hospitals in this city, which is no mean figure for a city of 300,000 inhabitants.
The number of consumptives who are brought in this way into a situation where they can no longer spread infection, is indeed fairly considerable and cannot remain without influence on the progress of this infectious disease.
In relation to this, I would like to draw your attention to a phenomenon which deserves the greatest consideration. This is the uniform and significant falling-off of the mortality due to consumption in several countries.
In England this decrease has already been under way for about 40 years. Significantly it is less in Scotland, and completely lacking in Ireland. The decline of tuberculosis in Prussia is very pronounced. During the decade 1876-1886 the mortality due to consumption still stood at a uniformly high level. Then from 1886 onwards, it fell from year to year, and has now dropped by more than 30%, i.e. by about a third. It has been calculated that, as a result of this, although the size of the population has risen in the meantime, each year about 20,000 fewer people will die of consumption in Prussia now than 20 years ago. In other countries, for example, Austria and Hungary, the mortality due to consumption has stayed at its former considerable level.
It is difficult to say what has brought about this characteristic behaviour of tuberculosis in the countries named. One supposes that several factors have worked together. The improvement in the situation of the lower strata of society, in particular with regard to housing conditions, and the improved knowledge of the risk of infection, which dissuades the individual from exposing himself unsuspectingly to infection any more, have certainly played their part in bringing about the decline in tuberculosis. But I am firmly convinced that the better provision for consumptives in the terminal stages, namely their accommodation in hospitals, which is happening to a relatively large extent in England and Prussia, has contributed most to the improvement in the tuberculosis situation. I am strengthened in this opinion particularly by the behaviour of tuberculosis in Stockholm, where, as has been mentioned already, proportionately many consumptives are cared for in institutions and where also the mortality due to consumption has decreased in the course of recent decades by 38%.
From this we must draw the lesson that the greatest emphasis must be placed on these measures in the fight against tuberculosis, namely on the accommodation of consumptives in suitable institutions, and much more care than before should be taken to insure that consumptives do not die in their homes, where they are moreover mostly in a helpless state, without adequate nursing.
When consumptives are no longer turned away, as before, by the hospitals as incurable, and when, on the contrary, we afford the best treatment conceivable and free of charge, and can even offer the prospect of a cure in a few cases, when in addition provision is made for their families during the illness, then there will be no need for any compulsion at all to make many more of these unfortunate sick people come to the hospitals, than is already happening now.
Now I am going to turn to the discussion of a measure which will combat tuberculosis in quite a different way. This is the matter of sanatoria. Sanatoria were established in the expectation that a great part, perhaps even the majority of consumptives can be cured in them. If this supposition were to be correct, then sanatoria would decidedly be one of the best weapons in the struggle against tuberculosis. But there is a good deal of argument as to the results of the sanatoria. By one side it is affirmed that they have had up to 70% of successful cures, while the other side disputes every success. Now it must be conceded that the 70% of successes does not refer to real cures, but only to the recovery of earning capacity. But from the standpoint of prophylaxis there is no gain in this, since a patient who is not completely cured but is only improved to the extent that he is capable of earning again for a while, later develops the condition of open tuberculosis, and succumbs to all its consequences, as were depicted earlier.
The reason for the relatively small number of real cures obtained in the sanatoria evidently lies in the fact that the duration of the treatment in these institutions is much too short, and that very many of the patients accepted are in such a far-advanced stage that the dietetic-hygienic treatment is no longer sufficient to cure them. Many doctors in sanatoria have also correctly recognized this already. For this reason they take care that only such patients are accepted as are in an early stage of tuberculosis, and in addition to the sanatorial treatment they administer tuberculin preparations, in order to achieve swifter, and, in particular, more lasting cures. In this way considerably better results than before have already been obtained in several sanatoria, and it is to be supposed that sanatoria, if they go on in this way, will make quite a substantial contribution to the fight against tuberculosis, at least in Germany, where already about 30,000 patients are now getting treatment each year in over a 100 sanatoria.
If in this way the greatest possible proportion of consumptives in an advanced state are taken care of by admission into the hospitals, and if the earliest stages of the disease are taken care of by the sanatoria, then there is still a large number of patients left, who must at all events be taken into account too. These are the ones in advanced stages of the disease who remain at home, and those consumptives whose illness has progressed too far for treatment in the sanatoria, but yet still not so far that they are incapable of working and have to go to a hospital. If these tuberculous people, whose numbers, as I have said, are truly considerable, are abandoned to their fate, then a great gap in the battle against tuberculosis would result from this.
To have filled in this gap is the merit of Calmette, who had the happy idea of taking care of this category of patient with the out-patient clinics which he had organized. This stimulus provided by Calmette has met with approval everywhere, especially in Germany, where over 50 such establishments have been set up, and many towns are on the point of providing themselves with them too. It was in Germany also that the out-patient clinics, which were originally only intended to provide the working-classes with free advice, medical treatment, and material support as well, were substantially broadened in scope and completed under the guidance of Pütter and Kayserling. In their present form they are intended not only to serve a particular class, but to serve all helpless sufferers from tuberculosis in every way. The sick person is visited in his home, and he and his relations are given instruction and advice concerning cleanliness and how to deal with expectorations. If living conditions are bad, then money is granted in order to make it possible to arrange the separation of the sick person from the healthy relatives in his house either by renting a suitable room or by supplying different, more adequate accommodation, and in this way to make the dangerous patient relatively harmless. In addition poor families are supported by granting them appropriate food, fuel, etc. The institute itself does not take over the treatment of the sick, so as not to come into conflict with the medical practitioners; but it sees to it that they come under medical treatment, and, where appropriate, that they gain admission to a hospital, sanatorium or convalescent home. But a particularly important aspect of their work consists in watching over the relatives, in particular the children, and in investigating from time to time to see whether infection has resulted, so as to be able to bring help as early as possible.
In such ways these institutes provide the poor consumptives with a true welfare service, and on this account, with full justification, they have been called “social welfare centers”. I consider these arrangements to be one of the most powerful weapons, if not the most powerful, which we can bring into use against tuberculosis, and I believe that the social welfare centres, if, as is to be hoped, they spread over the country in a close network, are destined to exercise an extremely beneficial effect.
The measures which have been mentioned so far, namely duty to registrate, hospitals, sanatoria, and social welfare centres, comprise the heavy artillery in the fight against tuberculosis. But besides these, other lighter weapons are available to us, which can not produce any such decisive effect on their own, but whose aid we cannot dispense with.
Among these I mention in the first place all the efforts which have been directed at instructing the people on the danger of tuberculosis by means of popular publications, lectures, exhibitions and other media of that kind, and at keeping alive the interest of all social classes in the fight against tuberculosis. Later, when the social welfare centres are available in sufficient numbers, instruction will be dispensed on such a generous scale from these institutes, that we will hardly need special arrangements for this any more then; but for the present we cannot dispense with them.
In addition the numerous societies and associations provide very valuable help, which participate in the fight against tuberculosis by supplying money with which to found sanatoria and convalescent homes, to endow free beds, and to support the families of poor consumptives, etc.
We should not close our eyes to the fact that the fight against tuberculosis needs quite considerable financial resources. Basically it is only a question of money. The more free beds for consumptives that are endowed in well-equipped and well-run sanatoria and nursing-homes, the more adequately the families of the tuberculous are supported, so that the sick are not dissuaded from going into hospital out of concern for their relatives, and the more social welfare centres are set up, the more rapidly will tuberculosis decrease in importance as a wide-spread infectious disease.
Since, however, it is hardly to be expected that communities, which have already now often made generous sacrifices on behalf of their tuberculous members, will be able to meet all the requirements in this respect in the immediate future, it follows that help coming from private quarters is much to be desired. But care must be taken that the funds raised by societies and associations, or made available by individual benefactors, do not find employment on matters of secondary importance, but that they should be used to further the most effective measures, above all the institutes for the accommodation of the sick and the social welfare centres.
In the fight against tuberculosis, as it has been depicted so far, hardly anything remains to be done by the State, and yet, for its part, it can contribute to it in an effective way. This can happen by the State introducing legislation for compulsory registration for tuberculosis, which already is in force for all the other important wide-spread infectious diseases. In several countries this has already happened, and it is to be hoped that the other civilized countries will soon follow this example. Often a legislative foundation as well has been required for the compulsory isolation of such sick people, who are particularly dangerous to those surrounding them. According to my experience in the fight against contagious diseases we can, however, dispense with these stem measures. If we only make the admission of consumptives into suitable hospitals easier in the way indicated earlier, then we will achieve all we need.
But the State can interfere particularly usefully in one respect, namely as regards the improvement of unfavourable housing conditions. Private action is virtually powerless against this nuisance, while the State can easily remedy the situation with suitable laws.
If we look back on what has happened in recent years in the fight against tuberculosis as wide-spread infectious disease, then we cannot help but gain the impression that quite an important beginning has been made.
The struggle against tuberculosis is not dictated from above, and has not always developed in harmony with the rules of science, but it has originated in the people itself, which has finally correctly recognized its mortal enemy. It surges forward with elemental power, sometimes in a rather wild and disorganized fashion, but gradually more and more finding the right paths.
The struggle has caught hold along the whole line and enthusiasm for the lofty aim runs so high that a slackening is no longer to be feared.
If the work goes on in this powerful way, then the victory must be won.
The Nobel Foundation's copyright has expired.Robert Koch – Biographical
Robert Koch was born on December 11, 1843, at Clausthal in the Upper Harz Mountains. The son of a mining engineer, he astounded his parents at the age of five by telling them that he had, with the aid of the newspapers, taught himself to read, a feat which foreshadowed the intelligence and methodical persistence which were to be so characteristic of him in later life. He attended the local high school («Gymnasium») and there showed an interest in biology and, like his father, a strong urge to travel.
In 1862 Koch went to the University of Göttingen to study medicine. Here the Professor of Anatomy was Jacob Henle and Koch was, no doubt, influenced by Henle’s view, published in 1840, that infectious diseases were caused by living, parasitic organisms. After taking his M.D. degree in 1866, Koch went to Berlin for six months of chemical study and there came under the influence of Virchow. In 1867 he settled, after a period as Assistant in the General Hospital at Hamburg, in general practice, first at Langenhagen and soon after, in 1869, at Rackwitz, in the Province of Posen. Here he passed his District Medical Officer’s Examination. In 1870 he volunteered for service in the Franco-Prussian war and from 1872 to 1880 he was District Medical Officer for Wollstein. It was here that he carried out the epoch-making researches which placed him at one step in the front rank of scientific workers.
Anthrax was, at that time, prevalent among the farm animals in the Wollstein district and Koch, although he had no scientific equipment and was cut off entirely from libraries and contact with other scientific workers, embarked, in spite of the demands made on him by his busy practice, on a study of this disease. His laboratory was the 4-roomed flat that was his home, and his equipment, apart from the microscope given to him by his wife, he provided for himself. Earlier the anthrax bacillus had been discovered by Pollender, Rayer and Davaine, and Koch set himself to prove scientifically that this bacillus is, in fact, the cause of the disease. He inoculated mice, by means of home-made slivers of wood, with anthrax bacilli taken from the spleens of farm animals that had died of anthrax, and found that these mice were all killed by the bacilli, whereas mice inoculated at the same time with blood from the spleens of healthy animals did not suffer from the disease. This confirmed the work of others who had shown that the disease can be transmitted by means of the blood of animals suffering from anthrax.
But this did not satisfy Koch. He also wanted to know whether anthrax bacilli that had never been in contact with any kind of animal could cause the disease. To solve this problem he obtained pure cultures of the bacilli by growing them on the aqueous humour of the ox’s eye. By studying, drawing and photographing these cultures, Koch recorded the multiplication of the bacilli and noted that, when conditions are unfavourable to them, they produce inside themselves rounded spores which can resist adverse conditions, especially lack of oxygen and that, when suitable conditions of life are restored, the spores give rise to bacilli again. Koch grew the bacilli for several generations in these pure cultures and showed that, although they had had no contact with any kind of animal, they could still cause anthrax.
The results of this painstaking work were demonstrated by Koch to Ferdinand Cohn, Professor of Botany at the University of Breslau, who called a meeting of his colleagues to witness this demonstration, among whom was Professor Cohnheim, Professor of Pathological Anatomy. Both Cohn and Cohnheim were deeply impressed by Koch’s work and when Cohn, in 1876, published Koch’s work in the botanical journal of which he was the editor, Koch immediately became famous. He continued, nevertheless, to work at Wollstein for a further four years and during this period he improved his methods of fixing, staining and photographing bacteria and did further important work on the study of diseases caused by bacterial infections of wounds, publishing his results in 1878. In this work he provided, as he had done with anthrax, a practical and scientific basis for the control of these infections.
Koch was still, however, without adequate quarters or conditions for his work and it was not until 1880, when he was appointed a member of the «Reichs-Gesundheitsamt» (Imperial Health Bureau) in Berlin, that he was provided, first with a narrow, inadequate room, and later with a better laboratory, in which he could work with Loeffler, Gaffky and others, as his assistants. Here Koch continued to refine the bacteriological methods he had used in Wollstein. He invented new methods – «Reinkulturen» – of cultivating pure cultures of bacteria on solid media such as potato, and on agar kept in the special kind of flat dish invented by his colleague Petri, which is still in common use. He also developed new methods of staining bacteria which made them more easily visible and helped to identify them. The result of all this work was the introduction of methods by which pathogenic bacteria could be simply and easily obtained in pure culture, free from other organisms and by which they could be detected and identified. Koch also laid down the conditions, known as Koch’s postulates, which must be satisfied before it can be accepted that particular bacteria cause particular diseases.
Some two years after his arrival in Berlin Koch discovered the tubercle bacillus and also a method of growing it in pure culture. In 1882 he published his classical work on this bacillus. He was still busy with work on tuberculosis when he was sent, in 1883, to Egypt as Leader of the German Cholera Commission, to investigate an outbreak of cholera in that country. Here he discovered the vibrio that causes cholera and brought back pure cultures of it to Germany. He also studied cholera in India.
On the basis of his knowledge of the biology and mode of distribution of the cholera vibrio, Koch formulated rules for the control of epidemics of cholera which were approved by the Great Powers in Dresden in 1893 and formed the basis of the methods of control which are still used today. His work on cholera, for which a Prize of 100,000 German Marks was awarded to him, also had an important influence on plans for the conservation of water supplies.
In 1885 Koch was appointed Professor of Hygiene in the University of Berlin and Director of the newly established Institute of Hygiene in the University there. In 1890 he was appointed Surgeon General (Generalarzt) Class I and Freeman of the City of Berlin. In 1891 he became an Honorary Professor of the Medical Faculty of Berlin and Director of the new Institute for Infectious Diseases, where he was fortunate to have among his colleagues, such men as Ehrlich, von Behring and Kitasato, who themselves made great discoveries.
During this period Koch returned to his work on tuberculosis. He sought to arrest the disease by means of a preparation, which he called tuberculin, made from cultures of tubercle bacilli. He made two preparations of this kind called the old and the new tuberculin respectively, and his first communication on the old tuberculin aroused considerable controversy. Unfortunately, the healing power that Koch claimed for this preparation was greatly exaggerated and, because hopes raised by it were not fulfilled, opinion went against it and against Koch. The new tuberculin was announced by Koch in 1896 and the curative value of this also was disappointing; but it led, nevertheless, to the discovery of substances of diagnostic value. While this work on tuberculin was going on, his colleagues at the Institute for Infectious Diseases, von Behring, Ehrlich and Kitasato, carried out and published their epoch-making work on the immunology of diphtheria (see the biographies of Ehrlich and von Behring).
In 1896 Koch went to South Africa to study the origin of rinderpest and although he did not identify the cause of this disease, he succeeded in limiting the outbreak of it by injection into healthy farm-stock of bile taken from the gall bladders of infected animals. Then followed work in India and Africa on malaria, blackwater fever, surra of cattle and horses and plague, and the publication of his observations on these diseases in 1898. Soon after his return to Germany he was sent to Italy and the tropics where he confirmed the work of Sir Ronald Ross in malaria and did useful work on the aetiology of the different forms of malaria and their control with quinine.
It was during these later years of his life that Koch came to the conclusion that the bacilli that caused human and bovine tuberculosis are not identical and his statement of this view at the International Medical Congress on Tuberculosis in London in 1901 caused much controversy and opposition; but it is now known that Koch’s view was the right one. His work on typhus led to the idea, then a new one, that this disease is transmitted much more often from man to man than from drinking water and this led to new control measures.
In December, 1904, Koch was sent to German East Africa to study East Coast fever of cattle and he made important observations, not only on this disease, but also on pathogenic species of Babesia and Trypanosoma and on tickborne spirochaetosis, continuing his work on these organisms when he returned home.
Koch was the recipient of many prizes and medals, honorary doctorates of the Universities of Heidelberg and Bologna, honorary citizenships of Berlin, Wollstein and his native Clausthal, and honorary memberships of learned societies and academies in Berlin, Vienna, Posen, Perugia, Naples and New York. He was awarded the German Order of the Crown, the Grand Cross of the German Order of the Red Eagle (the first time this high distinction was awarded a medical man), and Orders from Russia and Turkey. Long after his death, he was posthumously honoured by memorials and in other ways in several countries.
In 1905 he was awarded the Nobel Prize for Physiology or Medicine. In 1906, he returned to Central Africa to work on the control of human trypanosomiasis, and there he reported that atoxyl is as effective against this disease as quinine is against malaria. Thereafter Koch continued his experimental work on bacteriology and serology.
In 1866 Koch married Emmy Fraats. She bore him his only child, Gertrud (b. 1865), who became the wife of Dr. E. Pfuhl. In 1893 Koch married Hedwig Freiberg.
Dr. Koch died on May 27, 1910, in Baden-Baden.
This autobiography/biography was written at the time of the award and first published in the book series Les Prix Nobel. It was later edited and republished in Nobel Lectures. To cite this document, always state the source as shown above.
The Nobel Foundation's copyright has expired.Robert J. Lefkowitz – Biographical

ORIGINS
According to an article in The Times of Israel (issue of Dec. 9, 2012) by Mark Schulte, Dr. Alvin Roth (co-recipient of this year’s Nobel Prize in Economic Sciences) and I share two attributes with thirty-three other Nobel Laureates. We are Jewish and we were educated in New York City public high schools. This article further highlights the fact that “the overwhelming majority” of this group descended from “Eastern European Jews who came to America between 1881 and 1924, during the great migration.” In my case this was true of all four of my grandparents. My paternal grandparents, Mariam (Mary) Kremsdorf and Louis Lefkowitz, were from two nearby towns in southeast Poland, Czestochowa and Zoloshin. They were already married with one child when they immigrated to the United States in 1903, initially settling on the Lower East Side of Manhattan. They would live their entire lives in New York City, primarily in the Bronx and raise seven children, the second oldest of whom was my father, Max, (b. 1905). My grandfather was a cap maker and my grandmother, a homemaker.
My mother’s parents, Bernard and Rivka Levine, were from Russia and also immigrated to New York City. My mother, Rose, was the elder of their two daughters. My maternal grandmother’s family included several scholars and professionals. Her brother, Shlomo (Solomon) Polachek, was a famed rabbi and Talmudic scholar. Born in a small Russian village, he was known as a child prodigy at a young age and ultimately immigrated to the United States to become head of the Theological Seminary of Yeshiva University in New York City. One of his sons, Harry, was an ordained Rabbi and a prominent mathematician. The latter led him to become Technical Director of the Naval Applied Mathematics Lab, where he was an expert in early commercially available computers.
CHILDHOOD
I was born in 1943 and raised in the Bronx, in a high rise apartment complex known as Parkchester, the only child of Max, an accountant who worked in the garment district in Manhattan and Rose, an elementary school teacher. My mother was a high-strung perfectionist. She would check my homework for the slightest imperfection and demand that it be redone if she detected any flaws, which she invariably did. My father, in contrast, was easy going and affable and delighted in helping me with any project. He had a remarkable ability with numbers and could perform complex calculations in his head more rapidly than I could with pencil and paper. He would teach me many arithmetic manipulations and tricks several years before I would encounter them in school. When my absence of athletic ability manifested itself in an initial failure to meet required school standards for rope climbing and tumbling maneuvers, he insisted on setting up makeshift props at home and coaching me to ultimate success. As an adult, I can easily discern elements of both my parents’ personalities in myself.
As an only child lacking siblings and playmates, I was alone a great deal of the time. Much of this was spent reading virtually anything I could get my hands on. I began with my parents’ rather modest collection of volumes but then quickly discovered the local public library, from which I would regularly cart home the maximum allowable number of books (6 as I recall). I was rather precocious in this regard. I recall joining book clubs by sending in coupons I clipped from the newspapers which entitled me to claim a free set of books on the condition that an agreed upon number of additional volumes would be purchased over the next year. In this way I acquired, for example, Winston Churchill’s six-volume history, The Second World War, and Carl Sandberg’s six-volume biography of Abraham Lincoln. By the time I was about thirteen I had completed both sets. My parents, initially unaware of the contracts to which I had obligated them, were left to buy the remaining volumes, further adding to the family library. Increased time for reading these books was, on occasion, gained by faking illnesses such as abdominal cramps so that I could stay home from school and read all day.
My reading at this early stage also included numerous fiction and nonfiction titles related to medicine such as Sinclair Lewis‘ Arrowsmithand Paul de Kruif’s Microbe Hunters. My interest in these was sparked by my family physician, Dr. Joseph Feibush. By the third or fourth grade of elementary school I had decided that he was my occupational role model. I was enthralled by what he did, which included making routine house calls, performing physical exams, especially with a stethoscope, and writing illegible prescriptions. From then on I never wavered from my goal of studying medicine and becoming a physician.
Nonetheless, there were some early signs of interest in chemistry and biology as well. Among my favorite “toys” was my 1950s era chemistry set. Together with a friend we would follow the instructions in the manual, producing solutions of various colors or precipitates. We would copy out the experimental protocols from the guidebook into a notebook and make our own comments about what we saw. We told ourselves that we were creating a “chemistry textbook.” A “lab notebook” would have been a better description. A toy microscope of relatively low magnification was another favorite. Through it I viewed human hairs, insect parts of all sorts and a variety of prepared slides that came with the microscope set.
Lest I present myself as a totally bookish nerd at this stage (partial would be a better description), I hasten to point out that I enjoyed a wide range of activities typical of kids growing up in New York City during the 40s and 50s. These included stick ball, punch ball, trading baseball picture cards and riding bicycles. I was also an ardent fan of the New York Yankees major league baseball team (“the Bronx Bombers”) and can still repeat the batting order and uniform numbers of the teams from the early 1950s. I was active in the Boy Scouts and for many years took piano lessons, demonstrating relatively little talent. I played the drums, to the dismay of those living in neighboring apartments who would beat on the heating pipes to alert me that I was too loud. I was a member of the first generation of children to watch television, the earliest tiny sets arriving in some of my friends’ apartments when I was about five and in our home several years later. However, I can still remember listening to my favorite radio shows sitting on the floor in front of a large console radio.
One other influence which shaped me as a youngster was my participation in a family society called the Associated Kremsdorf Descendants (AKD’s). This family circle, consisting of the extended family of my paternal grandmother, would meet once a month for a meal, fellowship, entertainment and a formal business meeting. Complete with elected officers, committee reports and following strict rules of parliamentary procedure, these gatherings attracted dozens of family members from multiple generations. Such organizations were quite common among Eastern European immigrant Jewish families living in the northeast in the mid-20th century (as depicted in the movie “Avalon”). From these gatherings, which I greatly enjoyed, I gained a sense of the importance of family and a respect for, and appreciation of, the older members of the extended family who had all come from Europe.
EDUCATION
The Bronx High School of Science
After attending public elementary and junior high schools I entered The Bronx High School of Science (10th grade) in the autumn of 1956, graduating at age 16 in 1959. “Bronx Science” is one of several public high schools in New York City which admits students on the basis of a competitive examination. The student body, representing approximately the top 5% based on the exam, are gifted and interested in science and math. The accomplishments of graduates of this high school are quite remarkable. For example, I am the 8th Nobel Laureate to have graduated from this school, the 7 previous ones having received their prizes in Physics. For me, attending this school was a formative experience. Whereas in elementary and junior high school I was not greatly challenged, here I was among a group of remarkably bright, interesting and stimulating classmates. The curriculum featured many advanced classes at the college level. I was particularly drawn to chemistry and, as a result of taking these college level classes, I was able to receive full credit for two years of chemistry when I entered Columbia College in 1959. Thus I began as a college freshman with organic chemistry, a course generally taken by juniors.
The level of scholarship maintained by the student body was such that even with an average of about 94% my final class rank was about 100th out of 800. A classmate and friend at the time and at present, the famous geneticist David Botstein, had an almost identical average, a fact we tease each other about to this day.
College
Along with dozens of classmates, I moved on to Columbia University where I enrolled as a pre-medical student majoring in chemistry. The two year core curriculum in “Contemporary Civilization” was required of all students. With an emphasis on reading classic texts in history, philosophy, sociology and the political sciences and discussing these in small seminars, it was for me an opening to a whole new world. In addition, I took courses with and was exposed to, such intellectual giants as the literary critic Lionel Trilling, the cultural historian Jacques Barzun and the sociologist Daniel Bell, among others. I have very fond memories from this period of spending many hours in the public reading room at the 42nd Street New York Public Library, researching papers for those classes.
I also studied advanced Organic Chemistry with Cheves Walling and Physical Chemistry in a department which was strongly influenced by the then recently retired prominent physical organic chemist, Louis Hammett. However, the chemistry professor who had the most profound influence on me was actually a young Assistant Professor of Chemistry, Ronald Breslow. As a college senior I took an advanced seminar in biochemistry which he taught single handedly. This introduction to the chemistry of processes in living organisms really excited me in part, I suspect, because of his very lively teaching style. None of this, however, in any way diverted me from my goal of studying to become a practicing physician. In fact, by midway through my second year at Columbia it had become clear to me that, as a consequence of the credits I had received for college level courses taken in high school, I would be eligible for graduation after only three years. I needed only a couple of courses in summer school, graduating in 1962 at the age of 19, and moving uptown to the Columbia University College of Physicians and Surgeons.
Medical school
I greatly enjoyed my four years in medical school. I had dreamed about becoming a physician since grade school and now I was finally doing it. As a freshman immersed in the basic medical sciences I was able to deepen my interest in, and fascination with, biochemistry. Our biochemistry professors included a remarkable array of scholars (not that any of us appreciated that at the time). We heard lectures on metabolism from David Rittenberg, Chair of the Department; from David Shemin on porphyrins; from Erwin Chargaff on nucleic acids; and from David Nachmansohn on cholinergic neurotransmission. As stimulating as these subjects were to me, it was the clinical work that I was really pointing toward. Much as I enjoyed learning about biochemistry, at this stage the idea of actually doing research never entered my mind. In fact, although short blocks of time were available for research electives, I always chose clinical ones instead.
One young professor left a lasting impression on me. Paul Marks was then a young academic hematologist who taught the Introduction to Clinical Medicine course in which we studied clinical problems for the first time, examined case histories, and looked at blood specimens. Not only was he a good clinician but he assigned readings from the basic science literature that were relevant in a very meaningful way to the cases we studied. This showed me how scientific information could be brought to bear on clinical problems. Among my classmates and friends in medical school was Harold Varmus, who was the co-recipient of the 1989 Nobel Prize for the discovery of oncogenes.
At the end of my first year of medical school, I married Arna Gornstein and our first two children, David and Larry, were born in 1964 and 1965.
House staff
Upon graduation in 1966, I remained at Columbia for two years of house staff training in internal medicine at the Columbia Presbyterian Medical Center. This experience was intense, exhausting as well as exhilarating. I was doing what I had longed to do and I loved it, but I was not sleeping very much. As interns we followed a two week on call cycle in which one week was five nights on duty and two off, and the second was two nights on call and five off. “On call” meant that one slept in the hospital, though it was rare indeed to get more than a very few uninterrupted hours. It was not rare, however, to go two successive nights and intervening days with absolutely no sleep. This consistent sleep deprivation taught us what the limits of our endurance were and fostered a remarkable work ethic. However, it simultaneously degraded our performance at work and our ability to enjoy family time when at home, since the need to sleep overwhelmed all else. Needless to say, this schedule left precious little time for keeping up with the scientific or medical literature. Regulations now prevent working anything like these hours for house staff physicians.
At this time the Vietnam War was raging and there was general conscription with a separate “doctor draft” for physicians. Regardless of which branch of the service you joined, the only certainty was that you would spend a year in Vietnam. One way around directly participating in this very unpopular war, which was of particular interest to budding academic physicians, was to join the commissioned corps of officers in the United States Public Health Service and to be assigned for two years to clinical and laboratory duties at the National Institutes of Health in Bethesda, Maryland. Obtaining one of these commissions was extremely competitive at the time but, because of my strong academic record and recommendations, I was successful.
NIH
On July 1, 1968 I moved my family (now including the recently born Cheryl) to Rockville, Maryland to begin my research career at the NIH in nearby Bethesda, Maryland. I had been assigned, through a matching program, to work with Drs. Jesse Roth and Ira Pastan in the Clinical Endocrinology Branch of the National Institute of Arthritis and Metabolic Diseases (NIAMD), now known as NIDDK, the National Institute of Diabetes and Digestive and Kidney Diseases. I was a Clinical Associate, meaning that in addition to doing full time research ten months out of the year, for two months I also supervised a clinical endocrinology in-patient service. Because of this, I gained a remarkable exposure to unusual endocrine diseases which were under study at the time. An example of this was acromegaly.
It was the heyday of interest in second messenger signaling after the discovery of cAMP by Earl Sutherland. He would receive the Nobel Prize in Medicine and Physiology for this in 1971. One hormone after another was being shown to stimulate the enzyme adenylate cyclase thus increasing intracellular levels of cAMP. The idea that these different hormones might work through distinct receptors was talked about but was controversial. Moreover, at the time there were no direct methods for studying the receptors. I was assigned the challenging task of developing a radioligand binding method to study the putative receptors for adrenocorticotropic hormone (ACTH) in plasma membranes derived from an ACTH responsive adrenocortical carcinoma passaged in nude mice. Lacking any prior meaningful laboratory experience, I spent my first year failing at virtually everything I tried and not handling this very well.
Toward the end of 1968 I traveled with my family to New York City to spend the Thanksgiving holiday with family. I discussed my great frustration, unhappiness and lack of progress with my father. He counseled me to just “hang in there” while making plans to continue my clinical training in medicine and cardiology after the completion of my two year stint at the NIH. We agreed that I obviously was not cut out to be a scientist and besides I had always dreamed of being a physician anyway. This plan made good sense to me. Our conversation, however, turned out to be the last time I spoke with my father, who died several weeks later after suffering his fourth myocardial infarction at age 63. His death affected me deeply and I felt, in some odd way, a responsibility to fulfill the plan of my future career that he and I had devised together during our last conversation. His death, combined with my repeated failures in the laboratory during 1968–69, made this one of the most difficult years of my life.
Accordingly, over the next few months I made plans to move to the Massachusetts General Hospital (MGH), one of the Harvard teaching hospitals, in July 1970 for an additional year of medical residency followed by two years of cardiology fellowship. Then, during the summer of 1969, my experiments began to bear some fruit. I was successful in developing the binding assay for ACTH and over the next year wrote my first scientific papers and presented my findings at meetings for the first time. It was exhilarating and fun. For the first time I began to consider the possibility of a career that included a research component. These musings were moot, however, since by now I was committed to moving on to full-time clinical training in Boston.
Recently, two Nobel Laureates, Mike Brown and Joe Goldstein, published a brief essay discussing the remarkable number of Nobel Laureates (9 so far) who have in common the fact that they came to the NIH as physicians during the brief space between 1964–1972 for postdoctoral research training. (1)
They dissect the unique convergence of circumstances which may have been responsible for this extraordinary result, including the quality of basic science mentors on the full time NIH staff, the competitiveness of “the best and the brightest” to obtain these positions during the Vietnam War years, and the now bygone emphasis on teaching of basic sciences in medical schools in the 1960s.
I was particularly fortunate to have access to two physician scientists as mentors, individuals with very different styles and personalities. Jesse Roth was highly imaginative, creative and burned with an infectious enthusiasm for almost any experimental result. Ira Pastan, no less creative, was much more staid, methodical and critical of every result. He could always spot a crucial control I had left out of my experiment, thereby rendering the result essentially uninterpretable. In addition to guiding me through these early days of my scientific career, they provided ongoing support during the period of repeated failure. I owe to these two men my introduction to research in general and to receptor biology in particular. As with my parents, I can readily perceive aspects of both of their approaches in my own scientific investigation and mentoring.
Lineages among Nobel Laureates are often commented upon. In my case, Jesse Roth had trained with Solomon Berson and Rosalyn Yalow whose development of radioimmunoassay led to the Nobel Prize in Medicine and Physiology to Yalow (1977) after Berson’s untimely death in 1972. Moreover, training in Ira Pastan’s laboratory contemporaneously with me was my medical school and house staff classmate and future Nobel Laureate, Harold Varmus. Ira had himself trained in the lab of another NIH career scientist, Earl Stadtman, who also trained a future Nobel Laureate, Mike Brown.
Massachusetts General Hospital
A defining experience occurred during my first six months back in clinical service as a Senior Resident at MGH. I gradually became aware of the fact that I missed being in the lab. Deprived of my daily “fix” of data, I felt somehow unsatisfied. This, despite the fact that I was again enjoying the hectic pace of the clinical work. Upon completion of the first six months of my residency year I was entitled to choose clinical electives for the next six months. Instead, and in clear violation of hospital rules for resident physicians, I elected to start back in the laboratory. Dr. Edgar Haber, the Chief of Cardiology and a prominent immunochemist, allowed me to begin working in his lab. I was fascinated by receptors and what I saw as their potential to form the basis for a whole new field of research just waiting to be explored. I spent a great deal of time analyzing which receptor I should attempt to study. As an aspiring academic cardiologist I wanted to work on something related to the cardiovascular system. I also wanted a receptor known to be coupled to adenylate cyclase. I initially focused on two models, the cardiac glucagon and β-adrenergic receptors. However, my attention quickly became focused on the latter, for very practical reasons. Unlike the case for peptide hormones such as glucagon or ACTH, literally dozens, if not hundreds of analogs of adrenaline and noradrenaline, as well as their antagonists were available which could be chemically modified to develop the types of new tools which would need to be developed to study the receptors. These would include radioligands, photoaffinity probes, affinity chromatography matrices and the like. Moreover, the first β-adrenergic receptor blocker (“β-blocker”) had recently been approved for clinical use in the United States, adding further to the attractiveness of this target to me.
So in the early months of 1971 I began the quest to prove the existence of β-adrenergic receptors, to study their properties, to learn about their chemical nature, how they were regulated and how they functioned. This work has consumed me for the past forty years. Over the next several years in Boston, working mostly with membrane fractions derived from canine myocardium, I sought to develop radioligand binding approaches to tag the β-adrenergic receptors. I focused initially on the use of [3H]labeled catecholamines such as norepinephrine, which are agonists for the receptor. Specific saturable binding could be demonstrated, and I thought initially that we had developed a valid approach to label the receptors. However, it became increasingly clear over the next few years that the sites being labeled lacked many of the properties that would be expected for true physiological receptor binding sites. Coming to this realization was difficult.
During this time I also published some of the very first studies demonstrating GTP regulation of β-adrenergic receptor stimulated adenylate cyclase following after the work of Martin Rodbell on GTP regulation of glucagon sensitive adenylate cyclase. I was now a cardiology fellow. As at the NIH, nights on call were often spent in the lab doing experiments while hoping that my on call beeper would remain quiet. During these years, I had many stimulating and profitable discussions with Geoffrey Sharpe, a faculty member in the Nephrology Division with an interest in cell signaling and adenylate cyclase.
The period in Boston from 1970–1973 was one of the busiest in my life. In addition to my “day job” as a Medical Resident and Cardiology Fellow, I also worked several “moonlighting jobs” to help support my growing family (my fourth child, Mara, arrived in 1971). I worked in various emergency rooms, did physical exams for insurance companies, and even served as team physician for a high school football team for two seasons (they never won a game during this time).
In the summer of 1972, I was recruited by Duke University Medical Center to join their faculty to develop a program in “molecular cardiology.”This was to begin upon the completion of my fellowship at MGH in 1973. The overtures came from the Department of Medicine (Chair, Dr. James B. Wyngaarden), the Cardiology Division (Chief, Dr. Andrew Wallace) and the Department of Biochemistry (Chair, Dr. Robert Hill). I initially declined their offer but, when they subsequently raised the ante including an Associate Professor rank in Medicine, it seemed like an offer “I couldn’t refuse.” Now, my course was set to move to Duke in Durham, North Carolina, to begin my faculty career on July 1, 1973.
Duke
Arriving at Duke on July 1, 1973, with my wife and 4 children (ages 2–9), I proceeded to set up my lab in a brand new building, the Sands Bldg., on Research Drive. I would occupy this space for fifteen years before moving to the new CARL building. It was clear that we still needed to develop a radioligand binding assay for the β-adenergic receptors in order to be able to study them. This would ultimately take us close to another year. However, in work with postdoc Marc Caron in the spring of 1974, we succeeded in developing [3H]dihydroalprenolol. Contemporaneously, Gerald Aurbach at the NIH, and Alex Levitzki at the Hebrew University in Jerusalem also developed similar approaches using different radioligands. This was a watershed event because it finally opened the door to direct study of the receptors. Together with M.D./Ph.D. student Rusty Williams we developed comparable assays for the α-adrenergic receptors shortly thereafter. Over the next several years we developed a variety of tools such as photoaffinity probes and affinity chromatography matrices for the various adrenergic receptor subtypes as well as computer based analytical approaches for analyzing ligand binding data. These approaches greatly facilitated the discovery of new receptor subtypes and led to new ways of conceptualizing receptor G protein interactions (for example the ternary complex model).
During my first five years at Duke I juggled clinical and laboratory responsibilities, attending Cardiology clinic each week as well as making teaching rounds on the Medical Service. As the years passed I gradually reduced these clinical activities, but I continued to make teaching rounds until 2003. For the past 10 years I have not engaged in clinical work.
For the first 20 of my 40 year career at Duke, I focused on three essential questions about G protein coupled receptors: what is their chemical nature; how do they signal; how is their function regulated? This period included the isolation of all four of the then known adrenergic receptor subtypes; cloning of their cDNAs revealing the homology with rhodopsin and the existence of the much wider gene family of seven transmembrane G protein coupled receptors; the discovery of the arrestin and G protein coupled receptor kinase gene families, the products of which desensitize the receptors; and the discovery of constitutively active mutant receptors, now known to be the cause of a growing number of inherited and acquired diseases. Our early work with the adrenergic receptors provided a template upon which many labs were able to build, using the first sequences of these receptors and homology cloning techniques to rapidly build out the family of GPCRs to its current huge size of ~1,000 genes in humans. The sheer size of this family, including hundreds of olfactory receptors, was not anticipated.
The next 20 years, until the present, have been focused more on the β-arrestin proteins. Originally discovered in the context of their role in desensitizing receptors, we have found that they are also key molecules involved in receptor signaling and endocytosis. I have been particularly interested in the phenomenon of “biased agonism”at GPCRs. This term refers to the unexpected ability of some receptor ligands to stimulate some receptor-promoted responses while blocking others. Working initially with the angiotensin AngII1A receptor we found peptide ligands that could stimulate β-arrestin mediated signaling while serving as antagonists for G protein mediated responses (“β-arrestin-biased”). The existence of such biased ligands has important implications for both basic and clinical research. For example, it strongly implies that there must be multiple active conformations of the receptor which have now become the object of biophysical and structural studies. Moreover, this discovery suggests that such biased GPCR ligands might represent an entirely new class of drugs which might display more specific actions with fewer side effects. To try to develop such agents, about five years ago, I co-founded a company called Trevena with my Duke colleague Howard Rockman. Details of many of the discoveries mentioned above are provided in my Nobel Lecture.
Throughout my scientific career there have been a number of sources of special satisfaction. One has been the trainees whom I have mentored, more than 200 at this point. Many of these have gone on to distinguished careers in academia, biotechnology and the pharmaceutical industry. My co-recipient of the 2012 Nobel Prize in Chemistry, Brian Kobilka, joined my lab as a cardiology fellow in 1984 and left for Stanford in 1989. He played a major role in our cloning of the adrenergic receptors. Even during those early years in training he demonstrated an appetite for risk and the talent for developing bold, original technical approaches to difficult scientific problems which have characterized his independent career ever since. In a gratifying turn of events over the past several years, Brian and I have been collaborating again on several projects of mutual interest.
There is no way that I can acknowledge here the many other individuals whose work, in aggregate, was recognized by my Nobel Prize. However, during the 70s and 80s, Marc Caron was a long term partner and deserves special mention.
A second major source of satisfaction has been the rapid translation of many of our findings and techniques into practical consequences in drug development. GPCRs are one of the commonest targets of therapeutic drugs. Thus, the development of radioligand binding methods and associated computer based analytic techniques fundamentally altered the way in which drug candidates were screened and developed, as well as how receptor subtypes were discovered. The cloning of the receptors led to discovery (by others) of many new “orphan” receptor drug targets. More recently our discovery of so called “biased” ligands which can preferentially activate G protein or β-arrestin signaling has suggested an approach to development of more specific drugs with potentially fewer side effects. A special aspect of my career has been my relationship with the Howard Hughes Medical Institute. I became an HHMI Investigator 37 years ago in 1976, at a time when there were only about 50 Investigators. Today there are well over 300 and I am one of the two longest serving Investigators (the other being Richard Palmiter). The Institute’s “Investigator” based support, rather than the “project” based support of conventional grant funding agencies has given me great freedom over the years to pursue my research goals in an unfettered and very privileged way. My research has also been supported throughout my career with grants from the NIH.
Along the way to receipt of the Nobel Prize I have been fortunate to receive a number of other awards for my research. Among others, these include: The Gairdner Foundation International Award (1988); Bristol-Myers Squibb Award for Distinguished Achievement in Cardiovascular Research (1992); Fred Conrad Koch Award – The Endocrine Society (2001); Jessie Stevenson Kovalenko Medal of the USA National Academy of Sciences (2001); Institut de France – Fondation Lefoulon-Delalande Grand Prix for Science (2003); The National Medal of Science (2007); The Shaw Prize in Life Science and Medicine (2007); The Albany Medical Center Prize in Medicine and Biomedical Research (2007); Research Achievement Award, American Heart Association (2009); BBVA Foundation Frontiers of Knowledge Award (2010).
I have been elected to membership in the National Academy of Sciences, the Institute of Medicine of the National Academy of Sciences, the American Academy of Arts and Sciences, The American Society of Clinical Investigation and The Association of American Physicians.
PERSONAL LIFE
I have a strong family history of coronary artery disease, my father having died at age 63 of a myocardial infarction and my mother having suffered a myocardial infarction at age 57. Perhaps not surprisingly, I developed angina at age 50 and had quadruple bypass surgery in 1994. I have tried to minimize my risk factors as aggressively as I can with daily physical exercise, a vegetarian diet and appropriate medications.
I have five children with my first wife, Arna: David (b. 1964); Larry (now Noah Jordan)(b. 1965); Cheryl (b. 1968); Mara (b. 1971) and Joshua (b. 1977). At the time of this writing I have five grandchildren: (Maya, Jonah, Madeleine, Samantha and Ethan). I have been married to the former Lynn Tilley of Durham, North Carolina, since 1991.

My family has always been a great source of pride, love and support for me throughout my career. While there can be little doubt that my obsessive focus on my science somewhat limited the time I could spend with each of my children as they were growing up, I like to believe that my work ethic, passion and enthusiasm for my life’s work provided a valuable role model for them. I started my family when I was quite young. My eldest child, David, was born when I was only 21 and my youngest, Joshua, was born when I was 34. In consequence, I have had the pleasure and privilege of relating to them for many years as adults. Having all of them, their spouses and significant others, two of my grandchildren and my wife Lynn with me during the festivities of Nobel Week was a joyous experience which we will always remember (Fig. 1).
REFERENCES
1. Goldstein, J.L. and Brown, M.S., “A Golden Era of Nobel Laureates,” Science 338:1033– 34, 2012.
This autobiography/biography was written at the time of the award and later published in the book series Les Prix Nobel/ Nobel Lectures/The Nobel Prizes. The information is sometimes updated with an addendum submitted by the Laureate.
Revealing secrets on a tiny scale
The small matter of what everything is made from has long fascinated humankind. Microscopes have had a huge impact on our understanding of everything from the composition of materials to the building blocks of life. The work of a number of Nobel Prize laureates have allowed microscopes to evolve.
A fascinating microbial world
Peering into the plastic eyepiece of his toy microscope to take a closer look at a drop of pond scum, Randy Schekman was transported into a fascinating microbial world. Aged 12, he was determined to save money from odd jobs to buy his first professional microscope. But he couldn’t reach his goal as his mother kept borrowing money from his piggy bank.

“One Saturday I became so upset that, after mowing a neighbour’s lawn, I bicycled to the police station and announced to the desk officer that I wanted to run away from home because my mother took my money and I couldn’t use it to buy a microscope,” he said.
The desperate measures paid off: his parents picked him up from the police station and bought the microscope on their way home. It remained a “treasured possession” throughout Schekman’s school years.
Making the invisible, visible
The microscope’s ability to be an extension of the human eye has enabled scientists to make strides in biology and medicine since its invention in the 16th century. Around one century ago, a scientific breakthrough by Richard Zsigmondy led to the development of the ultramicroscope.
But it was not until Frits Zernike took a fresh look at how refraction gives rise to the image in a microscope that scientists could distinguish transparent specimens such as bacteria and cells without having to cleverly illuminate or stain them.
When light rays pass through transparent materials, such as biological specimens, there is a change in the phase of the light waves – the position of the wave crests in relation to one another – compared to an unimpeded light ray. Our eyes can’t detect this but these phase changes contain important information that can be used to visualise the material they have passed through.
Zernike worked out a way to make this phase change visible, and built the phase contrast microscope in the 1930s. His microscope was capable of enhancing the contrast of unstained, transparent specimens to reveal their inner workings in richer detail, revolutionising biological and medical research.
Despite being told by a major microscope manufacturer that his invention had “little practical value”, Zernike’s work had a massive impact that continues to be felt.
Phase contrast microscopes have enabled strides in biological and medical research to be made, especially in the fields of histology – the study of tissues and organs in the body – and cancer research. They also allow commercial products such as oils, drugs and textiles to be scrutinised.
Seeing life at an atomic level
Ernst Ruska also had to overcome criticism, which began at an early age. Yet, Ruska’s conviction and curiosity paid off when, as a young student in 1933, he developed the first electron microscope. By using a magnetic coil as a lens he harnessed electron beams – instead of light – to obtain images of extremely small objects. The resulting image had a resolution greater than that of light microscopes, which was a breakthrough for science.
His invention allowed the smallest objects, such as cell organelles, viruses, or atoms, to be examined.
Ruska helped commercialise his invention, so that mass-produced electron microscopes rapidly found applications within many areas of science.
The development of the electron microscope opened up a previously hidden world. Ruska was recognised with the Nobel Prize in Physics 1986, which he shared with Gerd Binnig and Heinrich Rohrer who also turned to electrons to design a new microscope.
Binnig and Rohrer’s scanning tunnelling microscope (STM) used a single atom-sized stylus to create a topographical map of a surface. They exploited the tunnelling effect, in which a current flows between the stylus and the surface only if they are close enough together, to visualise the surface’s peaks and troughs at the atomic level. Thanks to their advances, crystal surfaces, DNA molecules and viruses could be visualised, opening up new vistas to life around us.
Bringing optical microscopy into the nanodimension
Electron microscopes are incredibly powerful, but they cannot be used to image living cells because the electrons destroy the samples.
For a long time, an alternative – optical microscopy – was held back because scientists presumed that optical microscopes would never obtain a better resolution than half the wavelength of light, and could therefore not be used to visualise tiny objects such viruses and protein molecules in cells.
Eric Betzig, Stefan Hell and William Moerner, awarded the Nobel Prize in Chemistry 2014, used fluorescence to bypass this limit. Their work allowed the optical microscope to peer into the nanoworld. Nanoscopy – the ability to see past the optical limit of 200-300nm – revolutionised the field of cell biology. Theoretically, there is no longer any object too small to be studied.
Hell’s technique used fluorescent molecules to image nano-sized parts of a cell. From this he developed the stimulated emission depletion (STED) microscope, which he used at the turn of the millennium to image E. coli bacterium at a resolution never before achieved in an optical microscope.
Betzig and Moerner laid the foundation for a second method; single-molecule microscopy. It relies upon the possibility to turn the fluorescence of individual molecules on and off. Scientists image the same area multiple times, letting just a few interspersed molecules glow each time. Superimposing these images yields a dense super-image resolved at the nanoscale.
Nanoscopy is, among other things, being used to better understand the function of living nerve cells and neuronal circuits. Scientists are working on allowing continuous observation, so they could “film” the workings of “molecular machines” such as proteins, which could be used, for example, to design new drugs.
Bolstering biochemistry
The Nobel Prize in Chemistry 2017 recognised discoveries that contributed to the development of cryo-electron microscopy, which has enabled a new era of biochemistry.

Electron microscopes were only useful for imaging dead objects, because the powerful electron beam destroys biological material. But thanks to the work of Richard Henderson, Joachim Frank and Jacques Dubochet, researchers can now freeze biomolecules mid-movement and portray them at atomic resolution.
Cryo-electron microscopy builds on Henderson and Frank’s research using electron microscopes to visualise biological samples and Dubochet’s method of cooling the water around molecules so rapidly they can be imaged in their ‘natural’ form. Today the technique is being successfully applied to multiple scientific disciplines to reveal molecular insights that would otherwise not be achievable.
In medical research, it is used, for example, to observe the 3D outer shell structures of viruses, uncover the atomic structures of proteins associated with neurodegenerative diseases, and to determine the structure and interactions of proteins that play a significant role in cancer. Better understanding of such mechanisms could lead to the development of more effective treatments.

Focusing on the future
Numerous Nobel Prize laureates have used microscopes to make beneficial breakthroughs for humankind. The founder of modern bacteriology, Robert Koch, reportedly penned a letter to microscope manufacturer Carl Zeiss that read, “a large part of my success I owe to your excellent microscopes,” having discovered the bacilli that caused tuberculosis and cholera, and receiving the Nobel Prize in Physiology or Medicine in 1905.
Microscopes will doubtlessly help future laureates to experience their eureka moments and brilliant breakthroughs. They are more than just instruments, but gateways to other tiny worlds, that continue to enable revolutionary discoveries.
Microscopes and the Nobel Prize
Nobel Prize laureates mentioned in this article


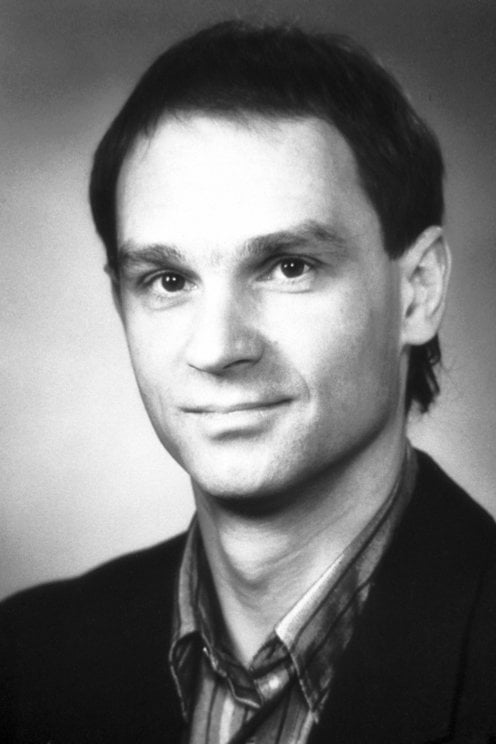
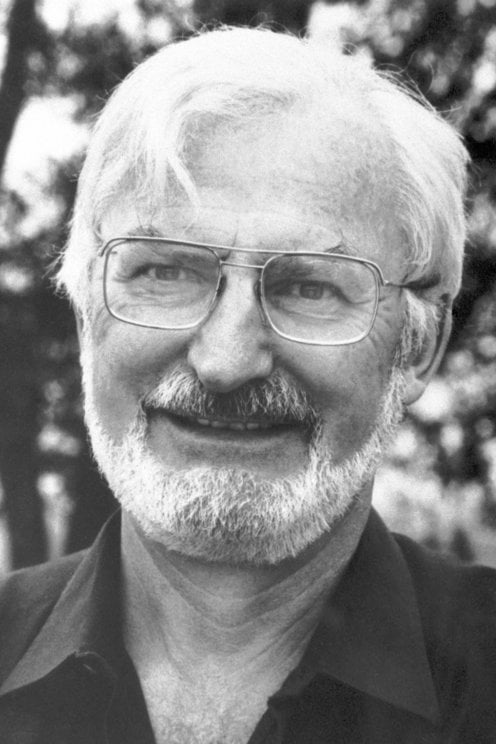






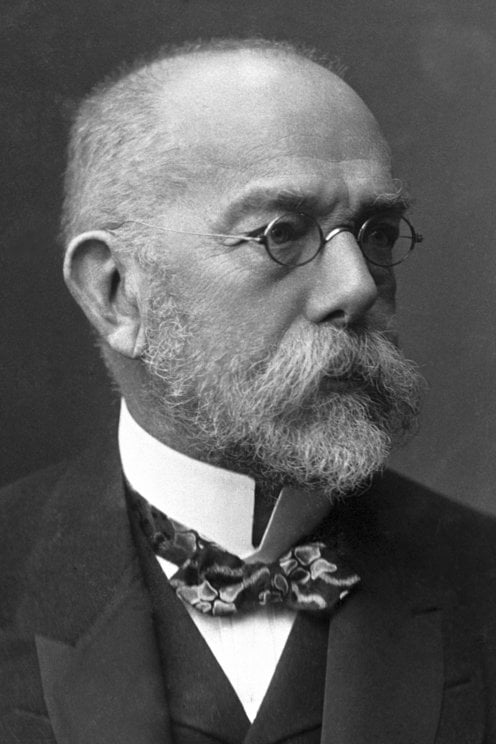
Michael Houghton – Biographical

Born in London, England in 1951 to Leonard George and Elsie Cressy Houghton, he was raised in a working-class family along with elder brother Graham. Educated at an excellent government primary school (Lyndhurst Grove) until the age of 11, he then won a scholarship to Alleyn’s School in Dulwich, London, founded by Edward Alleyn, a lead actor and producer of William Shakespeare’s plays in the 16th and 17th centuries. Graduating with college entry examinations in physics, chemistry and math, he decided to study biology at college, having been heavily influenced by reading at age 17 about the life and works of Louis Pasteur and also watching BBC TV coverage of the discovery of the DNA double helix early on Sunday mornings. In 1969, he entered the school of Biological Sciences at the new University of East Anglia, where he was highly motivated by the teachings of Professors Balls, Wilden and Thane as well as by full extracurricular activities including playing for the college cricket and squash teams. Offered attractive PhD positions at a London cancer research center, Oxford University, and Glasgow University, he failed to secure a stipend so entered the research laboratories of GD Searle & Co. in High Wycombe, UK, which was engaged in basic molecular biology research. Registering for a PhD in Biochemistry at King’s College, University of London in 1973 and co-supervised by Dr. Norman Carey (Searle) and Dr. James Chesterton (King’s), he graduated with a PhD in 1977 in a ceremony at the Alberta Hall with his wife, Han Fong Ida, who received her B. Pharm degree at the same ceremony from the London School of Pharmacy.
He then continued as a Research Investigator at Searle, benefiting from the excellent mentorship of Dr. Norman Carey and Dr. Richard Palmiter, where he characterized the human fibroblast interferon gene using newly emerging recombinant DNA technology. Offered many positions at burgeoning genetic engineering companies in the UK and US, in 1982 he chose to join the Chiron Corporation in California, founded by University of California Professors Bill Rutter and Ed Penhoet. Intending originally to work on chimeric type 1 interferons and to identify what became known later as type 3 interferons, he was introduced to the problem of Non-A, Non-B hepatitis by Dr. Dino Dina, then Director of Virology at Chiron. As a result, he decided to devote his laboratory to the pursuit of the causative agent(s) of this infectious disease, using a molecular biological approach, which was known not to be caused by the already charac- terized hepatitis A & B viruses. After pursuing numerous avenues unsuccessfully for many years, along with Dr. Qui-Lim Choo in his own laboratory, Chiron collaborator Dr. George Kuo, and CDC collaborator Dr. Dan Bradley, he published on the discovery of the hepatitis C virus (HCV) genome in 1989 with his collaborators, having published on the novel structure of the HDV genome in 1986. Following the HCV discovery, he and collaborators developed a series of patient diagnostics and blood screening tests that prevented post-transfusion hepatitis globally, as well as contributing to the identification of key enzymes crucial to the virus life cycle, which then became drug development targets for the field.
HCV infection represents a serious pandemic and so again with Dr. Choo and Dr. Kuo along with Dr. Ralston and others, he published the first evidence for an efficacious HCV vaccine in 1994 and subsequently performed 4 clinical trials in 3 different countries. His work has indicated the feasibility of developing an HCV vaccine, which he hopes to roll out to high-risk groups by the mid-2020s using both adjuvanted recombinant protein approaches as well as by applying the new RNA vaccine technologies at the Li Ka Shing Applied Virology Institute at the University of Alberta in Edmonton, Canada. He is also working with and supporting other leaders at the University of Alberta to develop a vaccine for Group A Streptococcus, and better drugs to treat Alzheimer’s disease and CMV infections. Now that HCV is a curable disease, he and others in the hepatology field are also turning their attention to the problem of non-alcoholic liver disease.
Education
1969–1972 BSc (Honors) Biological Sciences, University of East Anglia, Norwich, England
1973–1977 PhD Biochemistry, King’s College, University of London England
2019/7 Honorary Doctorate of Science University of East Anglia. Norwich, England
Positions
1977–1982 Research Investigator, Human Interferon Genetics, Searle Research Laboratories, Buckinghamshire, England
1982–1988 Project Leader, Non-A, Non-B Hepatitis Discovery Research, Chiron Corporation, Emeryville, CA
1988–2000 Director, Hepatitis C Research, Chiron Corporation, Emeryville, CA
2000–2003 Vice-President, Hepatitis C Research, Chiron Corporation, Emeryville, CA
2003–2006 Vice-President, Hepatitis C & Virology Research, Chiron Corporation, Emeryville, CA
2006–2007 Vice-President, Hepatitis C & Virology Research, Novartis Vaccines & Diagnostics, Inc., Emeryville, CA
2007–2009 Chief Scientific Officer, Epiphany Biosciences Inc., San Francisco, CA
2010–2018 Canada Excellence Research Chair in Virology and Li Ka Shing Professor, Department of Medical Microbiology and Immunology, University of Alberta Edmonton, AB, Canada
2013 – present Director of the Li Ka Shing Applied Virology Institute, University of Alberta, Edmonton, AB, Canada
Awards/Honors
The following honors were awarded for research on hepatitis C:
1992 Co-recipient of the Karl Landsteiner Award from the American Association of Blood Banks
1993 Co-recipient of the Robert Koch Medal from Germany
1993 Honoree of the Japanese Medical Congress
1993 Honoree of the Triennial International Hepatitis Meeting
1994 Co-recipient of the William Beaumont Prize from the American Gastroenterology Association
1994 Recipient of Beatrice Bitiello Award from Italian Association for Prevention of Viral Hepatitis
1994 Awardee of the Princess Takamatsu Cancer Research Fund from Japan
1998 Co-recipient of the International Hepatitis Foundation Award
1999 Co-recipient of the Hans Popper Award (Falk Foundation, Germany)
2000 Co-recipient of the Clinical Lasker Award (USA)
2005 Co-recipient of the Dale Smith Memorial Award of the American Association of Blood Banks
2009 Recipient of the Hepdart Lifetime Achievement Award (USA)
2011 Gold Medal from the Canadian Association for the Study of the Liver (CASL)
2011 The Australian Society for Microbiology Annual Scientific Meeting Bazeley Oration
2013 International Gairdner Award (Canada; declined)
2018 American Liver Foundation Distinguished Scientific Achievement Award (USA)
2020 The Nobel Prize in Medicine (The Nobel Foundation)
2021 Knighthood awarded by Queen Elizabeth II
Publications (by subject area and chronological order)
Transcriptional and Translational Control in Eukaryotes
Houghton M, Cox RF. (1974) The purification and properties of hen oviduct Form B DNA-dependent RNA polymerase. Nucl. Acids Res. 1:299–308.
Doel MT, Houghton M, Cook EA, Carey NH. (1977) The presence of ovalbumin mRNA coding sequences in multiple restriction fragments of chicken DNA. Nucl. Acids. Res. 4:3701–13.
Lilley DMJ, Houghton M. (1979) The interaction and RNA polymerase II from wheat with supercoiled and linear plasmid templates. Nucl. Acids. Res. 6:507–23.
Lilley DMJ, Jacobs MF, Houghton M. (1979) The nature of the interaction of nucleosomes with eukaryotic RNA polymerase II. Nucl. Acids Res. 7:377–99.
Lane CD, Colman A, Mohun T, Morser J, Champion J, Kourides I, Craig R, Higgins S, James TC, Applebaum SW, Ohlsson RI, Pauchas E, Houghton M, Matthews J, Miflin BJ. (1980) The Xenopus oocyte as a surrogate secretory system. Eur. J. Biochem. 111:225–35.
Sumikawa K, Houghton M, Emtage JS, Richards BM, Barnard EA. (1981) Active multi-subunit ACh receptor assembled by translation of heterologous mRNA in Xenopus oocytes. Nature. 292:862–4.
Sumikawa K, Houghton M, Smith JC, Bell L, Richards BM, Barnard EA. (1982) The molecular cloning and characterization of cDNA coding for the alpha subunit of the acetylcholine receptor. Nucl. Acids Res. 10:5809–22.
Kenten JH, Molgaard HV, Houghton M, Derbyshire RB, Viney J, Bell LO, Gould HJ. (1982) Cloning and sequence determination of the gene for the human immunoglobulin epsilon chain expressed in a myeloma cell line. Proc. Natl. Acad. Sci. USA. 79:6661–5.
Sumikawa K, Houghton M, Miledi R, Barnard EA. (1983) “A study of the mRNA and genes coding for the nicotinic acetylcholine receptor” in Cell Surface Receptors (Strange PG. ed.) pp. 249–69. Ellis Horwood Ltd., U.K.
Barnard EA, Houghton M, Miledi R, Richards BM, Sumikawa K. (1982) Molecular genetics of the acetyl choline receptor and its insertion and organization in the membrane. Biol. Cell. 45:383.
Molecular Genetics of Human Fibroblast Interferon
Houghton M, Stewart AG, Doel SM, Emtage JS, Eaton MAW, Smith JC, Patel TP, Lewis HM, Porter AG, Birch JR, Cartwright T, Carey NH. (1980) The amino– terminal sequence of human fibroblast interferon as deduced primers. Nucl. Acids Res. 8:1913–31.
Houghton M. (1980) Human interferon gene sequences. Nature. 285:536.
Houghton M, Eaton MAW, Stewart AG, Smith JC, Doel SM, Catlin GH, Lewis HM, Patel TP, Emtage JS, Carey NH, Porter AG. (1980) The complete amino acid sequence of human fibroblast interferon as deduced using synthetic oligodeoxyribonucleotide primers of reverse transcriptase. Nucl. Acids Res. 8:2885–94.
Houghton M, Jackson IJ, Porter AG, Doel SM, Catlin GH, Barber C, Carey NH. (1981) The absence of introns within a human fibroblast interferon gene. Nucl. Acids Res. 9:247–66.
Houghton M, Doel SM, Catlin GH, Stewart AG, Porter AG, Tacon WCA, Eaton MAW, Emtage JS, Carey NH. (1981) “The cloning and expression of a human fibroblast interferon gene in bacteria” in Proceedings of the Battelle International Genetic Engineering Conference (Keenberg M. ed.). Battelle Seminars and Studies Program.
McCullagh KG, Davies JA, Sim IS, Dawson KM, O’Neill GJ, Doel SM, Catlin GH, Houghton M. (1983) Biological properties of human interferon beta 1 synthesized in recombinant bacteria. J. Interf. Res. 3:97–111.
Porter AG, Bell LD, Adai JR, Catlin GH, Clarke JM, Davies JA, Dawson KM, Derbyshire RB, Doel SM, Dunthorne L, Finlay ME, Hall J, Houghton M, Hynes C, Lindley IJ, Nugent ME, O’Neill GJ, Smith JC, Stewart AG, Tacon WC, Viney JH, Warburton N, Boseley PG, McCullagh KG. (1985) “Active hybrids formed between human beta and alpha interferons” in The Biology of the Interferon System (Schellekers and Stewart eds.).
Porter AG, Bell LD, Adai JR, Catlin GH, Clarke JM, Davies JA, Dawson KM, Derbyshire RB, Doel SM, Dunthorne L, Finlay ME, Hall J, Houghton M, Hynes C, Lindley IJ, Nugent ME, O’Neill GJ, Smith JC, Stewart AG, Tacon WC, Viney JH, Warburton N, Boseley PG, McCullagh KG (1986) Novel modified beta interferons: gene cloning, expression and biological activity in bacterial extracts. DNA. 5:137–48.
Hepatitis Delta Virus
Wang KS, Choo QL, Weiner AJ, Ou JH, Najarian RC, Thayer RM, Mullenbach GT, Denniston KJ, Gerin JL, Houghton M. (1986) The structure, sequence and expression of the hepatitis delta (δ) viral genome. Nature. 323:508–14. Erratum in Nature. (1987) 328: 456.
Wang K-S, Choo Q-L, Weiner AJ, Ou J-H, Denniston KJ, Gerin JL, Houghton M (1987) “The Viroid-like structure of the hepatitis delta genome: synthesis of a viral antigen in recombinant bacteria” in The Hepatitis Delta Virus and its Infection (Rizzetto M, Gerin JL, Purcell RH. eds.) pp. 71–82. Alan Liss Inc., New York.
Weiner AJ, Wang K-S, Choo Q-L, Gerin JL, Bradley DW, Houghton M. (1987) Hepatitis delta (δ) cDNA clones: Undetectable hybridization to nucleic acids from infectious Non-A, Non-B hepatitis materials and hepatitis B DNA. J. Med. Virol. 21: 239–47.
Weiner AJ, Choo Q-L, Wang K-S, Govindarajan S, Redeker AG, Gerin JL, Houghton M. (1988) A single antigenomic open reading frame of the hepatitis delta virus encodes the epitope(s) of both hepatitis delta antigen polypeptides p24 delta and p27 delta. J. Virol. 62:594–9.
Weiner AJ, Choo Q-L, Wang K-S, Govindarajan S, Redeker AG, Gerin JL, Houghton M. (1988) A single antigenomic open reading frame of the hepatitis delta virus encodes the epitope(s) of both hepatitis delta antigen polypeptides p24 delta and p27 delta. J. Virol. 62:594–9.
Ponzetto A, Eckart M, D’Urso N, Negro F, Silvestro M, Bonino F, Wang KS, Chien D, Choo Q-L, Houghton M. (1993) Towards a vaccine for the prevention of hepatitis delta virus superinfection in HBV carriers. Prog. Clin. Biol. Res. 382:207–10.
Eckart MR, Dong C, Houghton M, D’Urso N, Ponzetto A. (1993) The effects of using recombinant vaccinia viruses expressing either large or small HDAg to protect woodchuck hepadnavirus carriers from HDV superinfection. Prog. Clin. Biol. Res. 382:201–05.
Nisini R, Paroli M, Accapezzato D, Bonino F, Rosina F, Santantonio T, Sallusto F, Amoroso A, Houghton M, Barnaba V. (1997) Human CD4+ T-cell response to hepatitis delta virus: identification of multiple epitopes and characterization of T-helper cytokine profiles. J. Virol. 71:2241–51.
Non-A, Non-B Hepatitis / Hepatitis C Virus
Choo Q-L, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M. (1989) Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 244:359–62.
Kuo G, Choo Q-L, Alter HJ, Gitnick GI, Redeker AG, Purcell RH, Miyamura T, Dienstag JL, Alter MJ, Stevens CE, Tegtmeier GE, Bonino F, Colombo M, Lee W-S, Kuo C, Berger K, Shuster JR, Overby LR, Bradley DW, Houghton M. (1989) An assay for circulating antibodies to a major etiologic virus of human non-A, non-B hepatitis. Science. 244:362–64.
Esteban JI, Viladomiu L, Bonzalez A, Roget M, Genesca J, Guardia J, Esteban R, Lopez-Talavera JC, Hernandez JM, Vargas V, Buti M, Kuo G, Choo Q-L, Houghton M. (1989) Hepatitis C virus antibodies among risk groups in Spain. Lancet. 334:294–7.
Van Der Poel CL, Ressink HW, Lelie PN, Leentvaar-Kuypers A, Choo Q-L, Kuo G, Houghton M. (1989) Anti-hepatitis C antibodies and non-A, non-B post-transfusion hepatitis in the Netherlands. Lancet. 334:297–8.
Parker T, de Medina M, Jeffers L, Reddy R, Bradley D, Schiff E, Houghton M, Choo Q-L, Kuo G. (1989) Hepatitis C virus HCV: A causative agent of cryptogenic cirrhosis CC among Cubans. Hepatology. 10:685.
Saracco G, Houghton M, Kuo G, Choo Q-L, Rosina F, Lattore V, Torrani Cerenzia MR, Chiandussi L, Bonino F, Rizzetto M. (1989) Anti-hepatitis C virus in non-A non-B patients responding and non-responding to alpha 2A interferon. J. Hepatol. 9:S219. Supplement 1.
Colombo M, Kuo G, Choo QL, Donato MF, Del Ninno E, Tommasini MA, Dioguardi N, Houghton M. (1989) Prevalence of antibodies to hepatitis C virus in Italian patients with hepatocellular carcinoma. Lancet. 334:1006–8.
Alter HJ, Purcell RH, Shih JW, Melpolder JC, Houghton M, Choo Q-L, Kuo G. (1989) Detection of antibody to hepatitis C virus in prospectively followed transfusion recipients with acute and chronic non-A, non-B hepatitis. N. Engl. J. Med. 321:1494–1500.
Takeuchi K, Boonmar S, Katayama T, Choo QL, Kuo G, Weiner AJ, Bradley DW, Houghton M, Saito I, Miyamura T. A cDNA fragment of hepatitis C virus isolated from an implicated donor of post-transfusion non-A, non-B hepatitis in Japan. Nucl. Acids Res. 17:10367–72.
Miyamura T, Saito I, Kubo Y, Takeuchi K, Boonmar S, Katayama T, Kuo G, Choo Q-L, Houghton M. (1989) “Hepatitis C virus complementary DNA clones isolated from a single healthy carrier who was shown to be an implicated donor of post-transfusion non-A, non-B hepatitis” in Proceedings of the International Meeting on Non-A, Non-B Hepatitis, Tokyo (Shikata T, Purcell RH, Uchida T. eds.) Elsevier Science Publishers, Amsterdam.
McHutchison JG, Kuo G, Houghton M, Choo Q-L, Redeker AG. (1989) Autoimmune hepatitis is not associated with antibodies to hepatitis C virus (HCV). Hepatology. 10:701.
Kamitsukasa H, Harada H, Yakura M, Fukuda A, Ohbayashi A, Saito I, Miyamura T, Choo Q-L, Houghton M, Kuo G. (1989) Intrafamilial transmission of hepatitis C virus. Lancet. 2:987. Letter.
Colombo M, Kuo G, Choo Q-L, Houghton M, Donato MF, Tommasini MA, Bargiggia S, Piva A, Del Ninno E, Dioguardi N. (1989) High prevalence of antibody to hepatitis C virus in patients with primary liver carcinoma. Hepatology. 10:700.
Colombo M, Kuo G, Choo Q-L, Houghton M, Tommasini MA, Rumi MG, Dioguardi ML, Donato MF, Del Ninno E. (1989) High prevalence of antibody to hepatitis C virus in patients with hepatocellular carcinoma HCC. J. Hepatol. 9:S20. Supplement 1.
Katkov WN, Cody H, Evans AA, Kuo G, Choo Q-L, Houghton M, Dienstag JL. (1989) The role of hepatitis C virus HCV in chronic liver disease. Hepatology. 10:644.
Katkov WN, Friedman LS, Cody H, Evans AA, Kuo G, Choo Q-L, Houghton M, Huggins CE, Dienstag JL. (1989) Elevated serum alanine aminotransferase ALT in blood donors: The contribution of hepatitis C virus HCV. Hepatology. 10:581.
McHutchison JG, Kuo G, Houghton M, Choo Q-L, Redeker AG. (1989) Circulating antibodies to hepatitis C virus HCV: A study of 160 cases of acute and chronic NANB hepatitis. Hepatology. 10:645.
Jeffers L, de Medina M, Hasan F, Reddy R, Parker T, Silva M, Mendez L, Schiff E, Houghton M, Choo Q-L, Kuo G. (1989) Hepatitis C HCV associated idiopathic chronic hepatitis and cryptogenic cirrhosis. Hepatology. 10:644.
Hasan F, Jeffers L, de Medina M, Reddy R, Parker T, Schiff E, Houghton M, Choo Q-L, Kuo G. (1989) Hepatitis C HCV associated hepatocellular carcinoma. Hepatology. 10:608.
Evans AA, Cody H, Kuo G, Choo Q-L, Houghton M, Katkov WN, Dienstag JL. (1989) Seroepidemiology of hepatitis C virus HCV in selected population. Hepatology. 10:644.
Krawczynski K, Kuo G, Dibisceglie A, Houghton M, Bradley DW. (1989) Bloodborne non-A, non-B hepatitis PT-NANB immunohistochemical identification of disease and hepatitis C virus-associated antigens. Hepatology. 10:580.
De Bisceglie AM, Alter H, Kuo G, Houghton M, Hoofnagle JH (1989) Detection of antibody to hepatitis C virus in patients with various chronic liver diseases.
Hepatology. 10:581.
Prince AM, Brotman B, Huima T, Krauledat P, Houghton M, Kuo G, Kuo Q-L. (1989) “Distinction between chronic and self-limited forms of hepatitis C virus infection” in International Meeting on Non-A, Non-B Hepatitis, Tokyo, Japan (Shikata T, Purcell RH, Uchida T. eds.) pp.7–16. Elsevier Science Publishers, Amsterdam.
Houghton M. (1990) Discovery of hepatitis C virus and assay of non-A, non-B hepatitis virus. Jikken Igaku. 8:203–6.
Mosley JW, Aach RD, Hollinger FB, Stevens CE, Barbosa LH, Nemo GJ, Holland PV, Bancroft WH, Zimmerman HJ, Kuo G, Choo Q-L, Houghton M. (1990) Non-A, non-B hepatitis and antibody to hepatitis C virus. JAMA. 263:77–8.
Weiner AJ, Kuo G, Bradley DW, Bonino F, Saracco G, Lee C, Rosenblatt J, Choo Q-L, Houghton M. (1990) Detection of hepatitis C viral sequences in non-A, non-B hepatitis. Lancet. 335:1–3.
Choo Q-L, Weiner AJ, Overby LR, Kuo G, Houghton M. (1990) Hepatitis C virus: The major causative agent of viral non-A, non-B hepatitis. Br. Med. Bull. 46:423–41.
Miyamura T, Saito I, Katayama T, Kikuchi S, Tateda A, Houghton M, Choo Q-L, Kuo G. (1990) Detection of antibody against antigen expressed by molecularly cloned hepatitis C virus cDNA: Application to diagnosis and blood screening for posttransfusion hepatitis. Proc. Natl. Acad. Sci. USA. 87:983–7.
Kew MC, Houghton M, Choo Q-L, Kuo G. (1990) Hepatitis C virus antibodies in southern African blacks with hepatocellular carcinoma. Lancet. 335:873–4.
Chien D-S, Kuo GC, Sung J-L, Lai M-Y, Sheu J-C, Chen P-J, Yang P-M, Hsu H-M, Chang M-H, Chen C-J, Hahn L-C, Choo Q-L, Wang T-H, Houghton M. (1990) Hepatitis C virus infection in an area hyperendemic for hepatitis B and chronic liver disease: The Taiwan experience. J. Infect. Dis. 162:817–22.
Makris M, Preston FE, Triger DR, Underwood JCE, Choo Q-L, Kuo G, Houghton M. (1909) Hepatitis C antibody and chronic liver disease in haemophilia. Lancet. 335:1117–9.
Stevens CE, Taylor PE, Pindyck J, Choo Q-L, Bradley DW, Kuo G, Houghton M. (1990) Epidemiology of hepatitis C virus. A preliminary study in volunteer blood donors. JAMA. 263:49–53.
Jeffers L, Perez G, de Medina M, Schiff E, Ortiz-Interian C, Bourgoignie J, Vaamonde CA, Houghton M, Choo Q-L, Kuo G. (1990) Hepatitis C HCV infection in hemodialysis units. Kidney Int. 37:303.
Oliveri F, Baldi M, Brunetto MR, Saracco G, Rosina F, Cerenzia MT, Rizzetto M, Soranzo ML, Colla L, Vallauri P, Verme G, Kuo G, Houghton M, Bonino F. (1990) Antibody to hepatitis C virus in the serum of patients with chronic hepatitis. Eur. J. Gastroenterol. Hepatol. 2:347–50.
Houghton M, Richman K, Han J, Berger K, Lee C, Dong C, Overby L, Weiner A, Bradley D, Kuo G, Choo Q-L. (1990) “Hepatitis C virus (HCV): A relative of the pestiviruses and flaviviruses” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 328–33. Williams & Wilkins, Baltimore, MD.
Choo Q-L, Berger K, Kuo G, Houghton M. (1990) “Detection and mapping of immunologic epitopes expressed by bacterial cDNA clones of the hepatitis C virus” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 345–6. Williams & Wilkins, Baltimore, MD.
Kuo G, Choo Q-L, Shuster J, Kuo C, Berger K, Lee WS, Medina-Selby A, Houghton M. (1990) “Serodiagnosis of hepatitis C viral infection using recombinant-based assays for circulating antibodies to different viral proteins” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 347–9. Williams & Wilkins, Baltimore, MD.
Weiner AJ, Truett MA, Rosenblatt J, Han J, Quan S, Polito AJ, Kuo G, Choo Q-L, Houghton M. (1990) “HCV: Immunologic and hybridization-based diagnostics” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 360–3. Williams & Wilkins, Baltimore, MD.
Boonmar S., Takeuchi K, Kubo Y, Katayama T, Harada H, Ohbayashi A, Choo Q-L, Kuo G, Houghton M, Saito I, Miyamura T. (1990) “Molecular cloning of hepatitis C virus cDNA from plasma of an implicated donor or post-transfusion non-A, non-B hepatitis” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 371–4. Williams & Wilkins, Baltimore, MD.
Shimizu YK, Weiner AJ, Rosenblatt J, Wong DC, Shapiro M, Popkin T, Houghton M, Alter HJ, Purcell RH. (1990) Early events in hepatitis C virus infection of chimpanzees. Proc. Natl. Acad. Sci. USA. 87:6441–4.
Van der Poel CL, Reesink HW, Lelie PN, Cuijpers MT, Leentvaar,-Kuypers A, Bakker E, Exel-Oehlers PJ, Polito A, Houghton M, Schaasberg W. (1990) “Impact of blood-donor screening for anti-HCV versus ALT, and cofactors for infectivity of anti-HCV-positive blood” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 427–30. Williams & Wilkins, Baltimore, MD.
Esteban JI, González A, Hernández JM, Madoz P, Muniz E, Torras J, Enriquez J, Buenestado J, Martin-Vega C, Sánchez C, Esteban R, Guardia J, Houghton M, Alter HJ. (1990) “Open prospective efficacy trial of anti-HCV screening of blood donors to prevent posttransfusion hepatitis: Interim report of the Barcelona PTH study” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 431–3. Williams & Wilkins, Baltimore, MD. Krawczynski K, Kuo G, Dibisceglie A, Bradley D, Houghton M, Alter M, Ebert J. (1990) “Blood-borne non-A, non-B hepatitis: Detection and identification of hepatitis C virus and disease-associated antigen HCV Ag in hepatocytes” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 434–5. Williams & Wilkins, Baltimore, MD.
Prince AM, Brotman B, Huima T, Krauledat P, Houghton M, Kuo G, Choo Q-L, Polito A, Di Nello R, Nelles MJ. (1990) Use of anti-HCV determinations for diagnosis of chronic HCV infection” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 450–5. Williams & Wilkins, Baltimore, MD.
Miyamura T, Saito I, Yoneyama T, Takeuchi K, Ohbayashi A, Watanabe Y, Choo Q-L, Houghton M, Kuo G. (1990) ‘Role of hepatitis C virus in hepatocellular carcinoma” in Viral Hepatitis and Liver Disease (Hollinger FB, Lemon SM, Margolis HS. eds.) pp. 559–62. Williams & Wilkins, Baltimore, MD.
Takeuchi K, Boonmar S, Kubo Y, Katayama T, Harada H, Ohbayashi A, Choo Q-L, Kuo G, Houghton M, Saito I, Miyamura T. (1990) Hepatitis C viral cDNA clones isolated from a healthy carrier donor implicated in post-transfusion non-A, non-B hepatitis. Gene. 91:287–91.
Watanabe J, Minegishi K, Mitsumori T, Ishifuji M, Oguchi T, Ueda M, Tokunaga E, Tanaka E, Kiyosawa K, Furuta S, Katayama T, Kuo G, Choo Q-L, Houghton M, Nishioka K. (1990) Prevalence of anti-HCV antibody in blood donors in the Tokyo area. Vox Sang. 59:86–8.
Katayama T, Kikuchi S, Tanaka Y, Saito I, Miyamura T, Choo Q-L, Houghton M, Kuo G. (1990) Blood screening for non-A, non-B hepatitis by hepatitis C virus antibody assay. Transfusion. 30:374–6.
Takeuchi K, Kubo Y, Boonmar S, Watanabe Y, Katayama T, Choo Q-L, Kuo G, Houghton M, Saito I, Miyamura T. (1990) The putative nucleocapsid and envelope protein genes of hepatitis C virus determined by comparison of the nucleotide sequences of two isolates derived from an experimentally infected chimpanzee and healthy human carriers. J. Gen. Virol. 71:3027–33.
Kremsdorf D, Thiers V, Garreau F, Duclos H, Porchon C, Houghton M, Tiollais P, Brechot C. (1990) Cloning and sequence analysis of hepatitis B virus variants in non-A and non-B infections. J. Hepatol. 11:S36. Supplement 2.
Saito I, Miyamura T, Ohbayashi A, Harada H, Katayama T, Kikuchi S, Watanabe Y, Koi S, Onji M, Ohta Y, Choo Q-L, Houghton M, Kuo G. (1990) Hepatitis C virus infection is associated with the development of hepatocellular carcinoma. Proc. Natl. Acad. Sci. USA. 87:6547–9.
Hasan F, Jeffers LJ, De Medina M, Reddy KR, Parker T, Schiff ER, Houghton M, Choo Q-L, Kuo G. (1990) Hepatitis C-associated hepatocellular carcinoma. Hepatology. 12:589–91.
Takeuchi K, Kubo Y, Boonmar S, Watanabe Y, Katayama T, Choo Q-L, Kuo G, Houghton M, Saito I, Miyamura T. (1990) Nucleotide sequence of core and envelope genes of the hepatitis C virus genome derived directly from human healthy carriers. Nuc. Acids Res. 18:4626.
Weiner AJ, Truett MA, Han J, Polito AJ, Choo, Q-L, Rosenblatt J, Quan S, Kuo G, Houghton M, Page E, Agius C, Nelles MJ. (1990) HCV testing in low-risk population. Lancet. 336:695. Letter.
Makris M, Dewar MS, Preston FE, Choo Q-L, Kuo G, Houghton M. (1990) The relation of hepatitis C antibodies to acute non-A, non-B hepatitis NANBH in previously untreated hemophilic patients. Br. J. Haematol. 74:44. Supplement 1.
Magrin S, Craxi A, Almasio P, Fabiano C, Fiorentino G, Palazzo U, Pinzello GB, Provenzano G, Pagliaro L, Houghton M, Han JH. (1990) HCV infection in autoimmune chronic active hepatitis. J. Hepatol. 11:S99. Supplement 2.
Thaler MM, Landers DW, Wara DW, Houghton M, Veereman-Wauters G, Sweet RL, Brauer M, Han JH. (1990) Vertical transmission of hepatitis C virus detected by the polymerase chain reaction. Hepatology. 12:849.
McHutchison JG, Kuo G, Houghton M, Choo Q-L, Redeker AG. (1990) Patients with acute and chronic NANB hepatitis. Hepatology. 12:966.
Leal RJ, McHutchison JG, Houghton M, Choo Q-L, Kuo G, Redeker AG. (1990) Antibodies to hepatitis C virus anti-HCV in alcoholic liver disease: An analysis of risk factors. Hepatology. 12:881.
Makris M, Preston FE, Triger DR, Underwood JCE, Kuo G, Choo Q-L, Houghton M. (1990) The role of hepatitis C virus in chronic liver disease in hemophilia. Br. J. Haematol. 74:6. Supplement 1.
Nishioka K, Watanabe J, Furuta S, Tanaka E, Suzuki H, Iino S, Tsuji T, Yano M, Kuo G, Choo Q-L, Houghton M, Oda T. (1991) Antibody to the hepatitis C virus in acute hepatitis and chronic liver diseases in Japan. Liver. 11:65–70.
Nishioka K, Watanabe J, Furuta S, Tanaka E, Iino S, Suzuki H, Tsuji T, Yano M, Kuo G, Choo Q-L, Houghton M, Oda T. (1991) A high prevalence of antibody to the hepatitis C virus in patients with hepatocellular carcinoma in Japan. Cancer. 67:429–33.
Katkov WN, Dienstag JL, Cody H, Evans AA, Choo QL, Houghton M, Kuo G. (1991) Role of hepatitis C virus in non-B chronic liver disease. Arch. Int. Med. 151:1548–52.
Choo Q-L, Han J, Weiner AJ, Overby LR, Bradley DW, Kuo G, Houghton M. (1991) “Hepatitis C virus is a distant relative of the flaviviruses and pestiviruses” in Proceedings of the International Meeting on Non-A, Non-B Hepatitis, Tokyo, Japan (Shikata T, Purcell RH, Uchida T. eds.) pp. 47–52. Elsevier Science Publishers, Amsterdam.
Di Bisceglie AM, Order SE, Klein JL, Wagoner JG, Sjogren MH, Kuo G, Houghton M, Choo Q-L, Hoofnagle JH. (1991) The role of chronic viral hepatitis in hepatocellular carcinoma in the United States. Am. J. Gastroenterol. 86:335–8.
Choo Q-L, Richman KH, Han JH, Berger K, Lee C, Dong C, Gallegos C, Coit D, Medina-Selby A, Barr PJ, Weiner AJ, Bradley DW, Kuo G, Houghton M. (1991) Genetic organization and diversity of the hepatitis C virus. Proc. Natl. Acad. Sci. USA. 88:2451–5.
Weiner AJ, Brauer MJ, Rosenblatt J, Richman KH, Tung J, Crawford K, Bonino F, Saracco G, Choo Q-L, Houghton M, Han JH. (1991) Variable and hypervariable domains are found in the regions of HCV corresponding to the flavivirus envelope and NS1 proteins and the pestivirus envelope glycoproteins. Virology. 180:842–8.
van der Poel CL, Cuypers HTM, Reesink HW, Weiner AJ, Quan S, DiNello R, van Boven JJP, Winkel I, Mulder-Folkerts D, Exel-Oehlers PJ, Schaasberg W, Leentvaar-Kuypers A, Polito A, Houghton M, Lelie PN. (1991) Confirmation of hepatitis C virus infection by new four-antigen recombinant immunoblot assay. Lancet. 337:317–9.
Reesink HW, Van der Poel CL, Plaisier ADD, Verstraten JW, Cuypers M. (1991) Comparison of first and second generation anti-HCV recombinant immunoblot assay with 5’ UTR PCR. Transfusion. 31:57S.
Han JH, Shyamala V, Richman KH, Brauer MJ, Irvine B, Urdea MS, Tekamp-Olson P, Kuo G, Choo Q-L, Houghton M. (1991) Characterization of the terminal regions of hepatitis C viral RNA: Identification of conserved sequences in the 5’ untranslated region and poly(A) tails at the 3’end. Proc. Natl. Acad. Sci. USA. 88:1711–5.
Magrin S, Craxi A, Fabiano C, Fiorentino G, Almasio P, Palazzo U, Pinzello G, Provenzano G, Pagliaro L, Choo Q-L, Kuo G, Polito A, Han J, Houghton M. (1991) Hepatitis C virus replication in ‘autoimmune’ chronic hepatitis. J. Hepatol. 13:364–7.
Cha T-A, Kolberg J, Irvine B, Stempien M, Beall E, Yano M, Choo Q-L, Houghton M, Kuo G, Han JH, Urdea MS. (1991) Use of a signature nucleotide sequence of Hepatitis C virus for detection of viral RNA in human serum and plasma. J. Clin. Microbiol. 29:2528–34.
Houghton M. (1991) “Molecular virology of HCV” in Report on the Proceedings, Second International Symposium on HCV, Los Angeles (Bradley DW. ed.) pp.2–3. Advanced Therapeutics Communications, Secaucus, New Jersey.
Krawczynski K, Beach M, Mimms L, Meeks E, Vallari D, Taskar S, Kuo G, Houghton M, Bradley D. (1991) Replication and antigenic expression of HCV antiviral antibody response and liver pathology in acute and chronic HCV infection. Hepatology. 14:78A.
Houghton M, Weiner A, Han J, Kuo G, Choo Q-L. (1991) Molecular biology of the hepatitis C viruses: Implications for diagnosis, development and control of viral disease. Hepatology. 14:381–8.
Colombo M, Rumi MG, Donato MF, Tommasini MA, Del Ninno E, Ronchi G, Kuo G, Houghton M. (1991) Hepatitis C antibody in patients with chronic liver disease and hepatocellular carcinoma. Dig. Dis. Sci. 36:1130–3.
Thudium K, Spaete R, Berger K, Choo Q-L, Houghton M, Ralston R. (1991) Expression and characterization of HCV structural proteins using in-vitro translation and recombinant vaccinia viruses. J. Cell. Biochem. 47:92. Supplement 15E.
McHutchison JG, Kuo G, Houghton M, Choo Q-L, Redeker AG. (1991) Hepatitis C virus antibodies in acute icteric and chronic non-A, non-B hepatitis. Gastroenterology. 101:1117–9.
Saracco G, Baldi M, Calvo PL, Manzini P, Abate M, Chiaberge E, Brunetto MR, Rizzetto M, Chien D, Kuo G, Houghton M, Bonino F. (1991) Hepatitis C virus markers for monitoring interferon therapy in chronic hepatitis C. Hepatology. 14:75A.
Cuypers HT, Winkel IN, van der Poel CL, Reesink HW, Lelie PN, Houghton M, Weiner A. (1991) Analysis of genomic variability of hepatitis C virus. J. Hepatol. 13:S15–9.
Rosina F, Fabiano A, Garripoli A, Smedile A, Mattalia A, Eckart MR, Houghton M, Bonino F. (1991) Rabbit-derived anti-HD antibodies for HDAg immunoblotting. J. Hepatol. 13:130–3.
Weiner AJ, Christopherson C, Hall JE, Bonino F, Saracco G, Crawford K, Marion CD, Crawford KA, Venkatakrishna S, Miyamura T, McHutchinson J, Cuypers T, Houghton M. (1991) Sequence variation in hepatitis C viral isolates. Hepatology. 13:S6–14.
Krawczynski K, Beach MJ, Bradley DW, Kuo G, di Bisceglie AM, Houghton M, Reyes GR, Kim JP, Choo Q-L, Alter MJ (1992) Hepatitis C virus antigen in hepatocytes: Immunomorphologic detection and identification. Gastroenterology. 103:622–9.
Bresters D, Mauser-Bunschoten EP, Cuypers HT, Lelie PN, Han JH, Jansen PL, Houghton M, Reesink HW (1992) Disappearance of hepatitis C virus RNA in plasma during interferon alpha-2B treatment in hemophilia patients. Scand. J. Gastroenterol. 27:166–8.
Bresters D, Cuypers HT, Reesink HW, Schaasberg WP, van der Poel CL, Mauser-Bunschoten EP, Houghton M, Choo Q-L, Kuo G, Lesniewski R, Troonen H, Lelie PN. (1992) Enhanced sensitivity of a second generation ELISA for antibody to hepatitis C virus. Vox Sang. 62:213–7.
Overby LR, Houghton M. (1992) “Hepatitis viruses” in Laboratory Diagnosis of Viral Infections (Lennette EH. ed.) pp. 403–44. Marcel Dekker, New York.
Spaete RR, Alexander DA, Rugroden ME, Choo Q-L, Berger K, Crawford K, Kuo C, Leng S, Lee C, Ralston R, Thudium K, Tung JW, Kuo G, Houghton M. (1992) Characterization of the hepatitis C virus E2/NS1 gene product expressed in mam-malian cells. Virology. 188:819–30.
Weiner AJ, Geysen HM, Christopherson C, Hall JE, Mason TJ, Saracco G, Bonino F, Crawford K, Marion CD, Crawford KA, Brunetto M, Barr PJ, Miyamura T, McHutchinson J, Houghton M. (1992) Evidence for immune selection of hepatitis C virus (HCV) putative envelope glycoprotein variants: Potential role in chronic HCV infections. Proc. Natl. Acad. Sci. USA. 89:3468–72.
Houghton M. (1992) “Heterogeneity of the HCV genome: Importance for control of the disease” in Hepatitis C Virus: Scientific and Clinical Status (Deinhardt F, Bradley DW, Houghton M. eds.) pp. 8–9. Advanced Therapeutics Communications, Secaucus, New Jersey.
Jeffers LJ, Hasan F, De Medina M, Reddy R, Parker T, Silva M, Mendez L, Schiff ER, Manns M, Houghton M. (1992) Prevalence of antibodies to hepatitis C virus among patients with cryptogenic chronic hepatitis and cirrhosis. Hepatology. 15:187–90.
Weiner AJ, Christopherson C, Hall JE, Crawford K, Marion CD, Crawford KA, Barr PJ, Richman K, Kuo G, Houghton M. (1992) “The hypervariable amino terminus of the hepatitis C virus E2/NS1 protein appears to be under immune selection” in Vaccines 92 (Brown F, Chanock RM, Ginsberg HS, Lerner RA. eds.) pp. 303–8. Cold Spring Harbor Laboratory Press, New York.
Chien DY, Choo Q-L, Tabrizi A, Kuo C, McFarland J, Berger K, Lee C, Shuster R, Nguyen T, Moyer DL, Tong M, Furuta S, Omata M, Alter H, Schiff E, Jeffers L, Houghton M, Kuo G. (1992) Diagnosis of hepatitis C virus (HCV) infection using an immunodominant chimeric polyprotein to capture circulating antibodies: Re-evaluation of the role of HCV in liver disease. Proc. Natl. Acad. Sci. USA. 89:10011–5.
Choo Q-L, Kuo G, Weiner A, Wang K-S, Overby L, Bradley D, Houghton M. (1992) Identification of the major, parenteral non-A, non-B hepatitis agent (hepatitis C virus) using a recombinant cDNA approach. Sem. Liver Dis. 12:279–88.
Cuypers HT, Bresters D, Winkel IN, Reesink HW Weiner AJ, Houghton M, van der Poel CL, Lelie PN. (1992) Storage conditions of blood samples and primer selection affect the yield of cDNA polymerase chain reaction products of hepatitis C virus. J. Clin. Microbiol. 30:3220–4.
Weiner AJ, Venkatakrishna S, Hall JE, Houghton M, Han J. (1992) “PCR: Application to hepatitis C virus (HCV) research and diagnostics” in Frontiers in Virology (Becker Y, Darai G. eds.) pp. 86–100. Springer Verlag, New York.
Van der Poel CL, Bresters D, Reesink HW, Plaisier AAD, Schaasberg W, Leentvaar-Kuypers A, Choo Q-L, Quan S, Polito A, Houghton M, Kuo G, Lelie PN, Cuypers HTM. (1992) Early antihepatitis-C virus response with second generation C200/C22 ELISA. Vox Sang. 62:208–12.
Han JH, Houghton M. (1992) Group specific sequences and conserved secondary structures at the 3’ end of HCV genome and its implication for viral replication. Nucl. Acids Res. 20:3520.
Koziel MJ, Dudley D, Wong JT, Dienstag J, Houghton M, Ralston R, Walker B. (1992) Intrahepatic cytotoxic T lymphocytes specific for hepatitis C virus in persons with chronic hepatitis. J. Immunol. 149:3339–44.
Yoo BJ, Spaete RR, Geballe AP, Selby M, Houghton M, Han JH. (1992) 5’ end-dependent translation initiation of hepatitis C viral RNA and the presence of putative positive and negative translational control elements within the 5’ untranslated region. Virology. 191:889–99.
Botarelli P, Brunetto MR, Weiner AJ, Minutello MA, Unutmaz D, Calvo P, Bonino F, Houghton M, Abrignani S. (1993) T cell response to recombinant proteins of hepatitis C virus in blood and liver of patients with different clinical courses of infection. Gastroenterology. 104:580–7.
Chien DY, Choo Q-L, Tabrizi A, Kuo C, McFarland J, Berger K, Lee C, Shuster JR, Nguyen T, Moyer DL, Tong M, Furuta S, Omata M, Fong CT, Tegtmeier G, Alter H, Schiff E, Jeffers L, Houghton M, Kuo G. (1993) Use of recombinant HCV antigen in the serodiagnosis of hepatitis C virus infection: Significant improvement in HCV antibody detection as compared with the first generation HCV C100-3 ELISA and the synthetic peptide EIA tests. J. Gastroenterol. Hepatol. 8:S33–9.
Eckart MR, Selby M, Masiarz F, Lee C, Berger K, Crawford K, Kuo C, Kuo G, Houghton M. (1993) The hepatitis C virus encodes a serine protease involved in processing of the putative nonstructural proteins from the viral polyprotein precursor. Biochem. Biophys. Res. Comm. 192:399–406.
Saracco G, Rosina F, Abate ML, Chiandussi L, Gallo V, Cerutti E, Di Napoli A, Solinas A, DePlano A, Tocco A, Cossu P, Chien D, Kuo G, Polito A, Weiner AJ, Houghton M, Verme G, Bonino F, Rizzetto M (1993) Long-term follow-up of patients with chronic hepatitis C treated with different doses of interferon-α2b. Hepatology. 18:1300–5.
Koziel MJ, Dudley D, Afdhal N, Choo Q-L, Houghton M, Ralston R, Walker BD. (1993) Hepatitis C virus (HCV)-specific cytotoxic T lymphocytes recognized epitopes in the core and envelope proteins of HCV. J. Virol. 67:7522–32.
Bresters D, Mauser-Bunschoten EP, Cuypers HT, Han JH, Jansen PL, Chamuleau RA, Houghton M, Reesink HW. (1993) Long term treatment of chronic hepatitis C with interferon alfa-2b: disappearance of HCV-RNA in a pilot study of eight haemophilia patients. Gut (England). 34:S124–5.
Rosina F, Fabiano A, Maran E, Cozzolongo R, Smedile A, Mazzucco G, Garripoli A, Costa C, Eckart MR, Houghton M. (1993) Rabbit-derived anti-HD antibodies for HDAg immunoblotting. Proc. Clin. Biol. Res. 382:189–91.
Selby MJ, Choo Q-L, Berger K, Kuo G, Glazer E, Eckart M, Lee C, Chien D, Kuo C, Houghton M. (1993) Expression, identification and subcellular localization of the proteinsencoded by the hepatitis C viral genome. J. Gen. Virol. 4:1103–13.
Weiner AJ, Thaler MM, Crawford K, Ching K, Kansopon J, Chien DY, Hall JE, Hu F, Houghton M. (1993) A unique, predominant hepatitis C virus variant found in an infant born to a mother with multiple variants. J. Virol. 67:4365–8.
Minutello MA, Pileri P, Unutmaz D, Censini S, Kuo G, Houghton M, Brunetto MR, Bonino F, Abrignani S. (1993) Compartmentalization of T lymphocytes to the site of disease: Intrahepatic CD4+ T cells specific for the protein NS4 of hepatitis C virus in patients with chronic hepatitis C. J. Exp. Med. 178:17–25.
Lok ASF, Chien D, Choo Q-L, Chan T-M, Chiu EKW, Cheng IKP, Houghton M, Kuo G. (1993) Antibody response to core, envelope and nonstructural hepatitis C virus antigens: Comparison of Immunocompetent and immunosuppressed patients. Hepatology. 18:497–502.
Chien DY, Choo Q-L, Ralston R, Spaete R, Tong M, Houghton M, Kuo G. (1993) Persistence of HCV despite antibodies to both putative envelope glycoprotein. Lancet. 342:933. Letter.
Erickson AL, Houghton M, Choo Q-L, Weiner AJ, Ralston R, Muchmore E, Walker CM. (1993) Hepatitis C virus-specific CTL responses in the liver of chimpanzees with acute and chronic hepatitis C. J. Immunol. 151:4189–99.
Ralston R, Thudium K, Berger K, Kuo C, Gervase B, Hall J, Selby M, Kuo G, Houghton M, Choo Q-L. (1993) Characterization of hepatitis C virus envelope glycoprotein complexes expressed by recombinant vaccinia viruses. J. Virol. 67:6753–61.
Botarelli P, Brunetto MR, Minutello MA, Calvo P, Unutmaz D, Weiner AJ, Choo Q-L, Shuster JR, Kuo G, Bonino F, Houghton M, Abrignani S. (1993) T-lymphocyte response to hepatitis C virus in different clinical courses of infection. Gastroenterology. 104:580–7.
Choo Q-L, Kuo G, Ralston R, Weiner A, Chien D, Van Nest G, Han J, Berger K, Thudium K, Kuo C, Kansopon J, McFarland J, Tabrizi A, Ching K, Moss B, Cummins LB, Houghton M, Muchmore E. (1994) Vaccination of chimpanzees against infection by the hepatitis C virus. Proc. Natl. Acad. Sci. USA. 91:1294–8.
Simmonds P, Alfredo A, Alter HJ, Bonino F, Bradley DW, Brechot C, Brouwer JT, Chan S-W, Chayama K, Chen D-S, Choo Q-L, Colombo M, Cuypers HTM, Date T, Dusheiko GM, Esteban JI, Fay O, Hadziyannis SJ, Han J, Hatzakis A, Holmes EC, Hotta H, Houghton M, Irvine B, Kohara M, Kolberg JA, Kuo G, Lau JYN, Lelie PN, Maertens G, McOmish F, Miyamura T, Mizokami M, Nomoto A, Prince AM, Reesink HW, Rice C, Roggendorf M, Schalm SW, Shimotohno K, Stuyver L, Trépo C, Weiner A, Yap PL, Urdea MS. (1994) A proposed system for the nomenclature of hepatitis C viral genotypes. Hepatology. 19:1321–4.
Houghton M, Selby M, Weiner A, Choo Q-L. (1994) Hepatitis C virus: Structure, protein products and processing of the polyprotein precursor. Curr. Stud. Hematol. Blood Trans. 61:1–11.
Houghton M, Choo Q-L, Kuo G, Ralston R, Selby M, Weiner A, Chien D, Han J, Walker C, Abrignani S, Koziel M, Walker B, Cummins L, Muchmore E. (1994) “The hepatitis C virus: Genetic organization, persistence, and vaccine strategies” in Viral Hepatitis and Liver Disease (Nishioka K, Suzuki H, Mishiro S, Oda T. eds.) pp. 33–7. Springer-Verlag, Tokyo.
Weiner AJ, Thaler MM, Crawford K, Kansopon J, Ching K, Hall JE, Hu F, Chien D, Houghton M. (1994) “HCV-positive, HIV-1-negative mothers transmit HCV” in Viral Hepatitis and Liver Disease (Nishioka K, Suzuki H, Mishiro S, Oda T. eds.) pp. 463–7. Springer-Verlag, Tokyo.
Ray R, Khanna A, Lagging LM, Meyer K, Choo Q-L, Ralston R, Houghton M, Becherer PR. (1994) Peptide immunogen mimicry of putative E1 glycoprotein-specific epitopes in hepatitis C virus. J. Virol. 68:4420–6.
Selby MJ, Glazer E, Masiarz F, Houghton M. (1994) Complex processing and protein: Protein interactions in the E2:NS2 region of HCV. Virology. 204:114–22.
Saracco G, Abate ML, Baldi M, Calvo PL, Manzini P, Brunetto MR, Oliveri F, Kuo G, Chien D, Houghton M, Verme G, Rizzetto M, Bonino F. (1994) Hepatitis C virus markers in patients with long-term biochemical and histological remission of chronic hepatitis. Liver. 14:65–70.
Chien DY, McFarland J, Tabrizi A, Kuo C, Houghton M, Kuo G. (1994) “Distinct subtypes of hepatitis C virus defined by antibodies directed to the putative core, NS4, and NS5 region polypeptides” in Viral Hepatitis and Liver Disease (Nishioka K, Suzuki H, Mishiro S, Oda T. eds.) pp. 320–4. Springer-Verlag, Tokyo.
Yoo BJ, Selby MJ, Choe J, Suh BS, Choi SH, Joh JS, Nuovo GJ, Lee H-S, Houghton M, Han JH. (1995) Transfection of a differentiated human hepatoma cell line (Huh7) with in vitro-transcribed hepatitis C virus (HCV) RNA and establishment of a long-term culture persistently infected with HCV. J. Virol. 69:32–8.
Cerny A, McHutchison JG, Pasquinelli C, Brown ME, Brothers MA, Grabscheid B, Fowler P, Houghton M, Chisari FV. (1995) Cytotoxic T lymphocyte response to hepatitis C virus – derived peptides containing the HLA A2.1 binding motif. J. Clin. Invest. 95:521–30.
Weiner A, Erickson AL, Kansopon J, Crawford K, Muchmore E, Hughes AL, Houghton M, Walker CM (1995) Persistent hepatitis C virus infection in a chimpanzee is associated with emergence of a cytotoxic T lymphocyte escape variant. Proc. Natl. Acad. Sci. USA. 92:2755–9.
Cerny A, Fowler P, Brothers MA, Houghton M, Schlicht HJ, Chisari FV. (1995) Induction in vitro of a primary human antiviral cytotoxic T cell response. Eur. J. Immunol. 25:627–30.
Houghton M, Choo Q-L, Kuo G, Weiner A, Chien D, Ralston R, Urdea M, Moss B, Purcell R, Cummins L, Muchmore E. (1995) Prospects for prophylactic and therapeutic hepatitis C virus vaccines. Princess Takamatsu Symp. 25:237–43.
Weiner AJ, Erickson AL, Kansopon J, Crawford K, Muchmore E, Houghton M, Walker CM. (1995) Association of cytotoxic T lymphocyte (CTL) escape mutations with persistent hepatitis C virus (HCV) infection. Princess Takamatsu Symp. 25:227–35.
Lagging LM, Meyer K, Hoft D, Houghton M, Belshe RB, Ray R. (1995) Immune responses to plasmid DNA encoding the hepatitis C virus core protein. J. Virol. 69:5859–63.
Koziel MJ, Dudley D, Afdhal N, Grakoui A, Rice C, Choo Q-L, Houghton M, Walker BD. (1995) HLA class I-restricted cytotoxic T lymphocytes specific for hepatitis C virus: Identification of multiple epitopes and characterization of patterns of cytokine release. J. Clin. Invest. 96:2311–21.
Piazza M, Chien D, Quan S, Houghton M. (1996) Lack of antibodies to the envelope glycoproteins of hepatitis C virus in immunoglobulin preparations from screened donors. Boll. Soc. Ital. Biol. Sper. 72:69–70.
Houghton M. (1996) “Hepatitis C viruses” in Fields Virology (Fields BN, Knipe DM, Howley PM et al. eds.) pp. 1035–58. Lippincott-Raven Publishers, Philadelphia.
Rosa D, Campagnoli S, Moretto C, Guenzi E, Cousens L, Chin M, Dong C, Weiner AJ, Lau JY, Choo Q-L, Chien D, Pileri P, Houghton M, Abrignani S. (1996) A quantitative test to estimate neutralizing antibodies to the hepatitis C virus: cytofluorimetric assessment of envelope glycoprotein 2 binding to target cells. Proc. Natl. Acad. Sci. USA. 93:1759–63.
Missale G, Bertoni R, Lamonaca V, Valli A, Massari M, Mori C, Rumi MG, Houghton M, Fiaccadori F, Ferrari C. (1996) Different clinical behaviors of acute hepatitis virus infection are associated with different vigor of the anti-viral cell-mediated immune response. J. Clin. Invest. 98:706–14.
Rehermann B, Chang KM, McHutchinson JG, Kokka R, Houghton M, Chisari FV. (1996) Quantitative analysis of the peripheral blood cytotoxic T lymphocyte response in patients with chronic hepatitis C virus infection. J. Clin. Invest. 98:1432–40.
Rehermann B, Chang KM, McHutchinson J, Kokka R, Houghton M, Rice CM, Chisari FV. (1996) Differential cytotoxic T-lymphocyte responsiveness to the hepatitis B and C viruses in chronically infected patients. J. Virol. 70:7092–102.
Houghton M, Choo Q-L, Chien D, Kuo G, Weiner A, Coates S, Cousens L, Wininger M, Selby M, Ralston R, Berger K, Dong C, Crawford K, Kansopon J, Chin M, Wong S, Tabrizi-Weight A, Purcell RH, Muchmore E, Morandi M, Rosa D, Abrignani S. (1996) “Development of an HCV vaccine” in Viral Hepatitis and Liver Disease (Rizzetto M, Purcell RH, Gerin JL, Verme G. eds.) pp. 656–9. Edizioni Minerva Medica, Torino, Italy.
Nelson DR, Marousis CG, Davis GL, Rice CM, Wong J, Houghton M, Lau YN (1997) The role of hepatitis C virus-specific cytotoxic T lymphocytes in chronic hepatitis C. J. Immunol. 158:1473–81.
Pasquinelli C, Shoenberger JM, Chung J, Chang KM, Guidotti LG, Selby M, Berger K, Lesniewski R, Houghton M, Chisari FV. Hepatitis C virus core and E2 protein expression in transgenic mice. Hepatology. 25:719–27.
Diepolder HM, Gerlach J-T, Zachoval R, Hoffmann RM, Jung M-C, Wierenga EA, Scholz S, Santantonio T, Houghton M, Southwood S, Sette A, Pape GR. (1997) Immunodominant CD4+ T-cell epitope within nonstructural protein 3 in acute hepatitis C virus infection. J. Virol. 71:6011–9.
Calvo PL, Kansopon J, Sra K, Quan S, DiNello R, Guaschino R, Calabrese G, Danielle F, Brunetto, Bonino F, Massaro AL, Polito A, Houghton M, Weiner AJ. (1998) Hepatitis C virus heteroduplex tracking assay for genotype determination reveals diverging genotype 2 isolates in Italian hemodialysis patients. J. Clin. Microbiol. 36:227–33.
Wong DKH, Dudley DD, Afdhal NH, Dienstag J, Rice CM. (1998) Liver-derived CTL in hepatitis C virus infection: Breadth and specificity of responses in a cohort of persons with chronic infection. J. Immunol. 160:1479–88.
Ishii K, Rosa D, Watanabe Y, Katayama T, Harada H, Wyatt C, Kiyosawa K, Aizaki H, Matsuura Y, Houghton M, Abrignani S, Miyamura T. (1998) High titers of antibodies inhibiting the binding of envelope to human cells correlate with natural resolution of chronic hepatitis C. Hepatology. 28:1117–20.
Pileri P, Uematsu Y, Campagnoli S, Galli G, Falugi F, Petracca R, Weiner AJ, Houghton M, Rosa D, Grandi G, Abrignani S. (1998) Binding of hepatitis C virus to CD81. Science. 282:938–41.
Selby M, Erickson A, Dong C, Cooper S, Parham P, Houghton M, Walker CM. (1999) Hepatitis C virus envelope glycoprotein E1 originates in the endoplasmic reticulum and requires cytoplasmic processing for presentation by class I MHC molecules. J. Immunol. 162:669–76.
Cooper S, Erickson AL, Adams EJ, Kansopon J, Weiner AJ, Chien DY, Houghton M, Parham P, Walker CM. (1999) Analysis of a successful immune response against hepatitis C virus. Immunity. 10:439–49.
Colombatto P, Brunetto MR, Kansopon J, Oliveri F, Maina A, Aragon U, Bortoli ML, Scatena F, Baicchi U, Houghton M, Bonino F, Weiner AJ. (1999) High prevalence of G1 and G2 TT-virus infection in subjects with high and low blood exposure risk: identification of G4 isolates in Italy. J. Hepatol. 31:990–6.
Abrignani S, Houghton M, Hsu HH. (1999) Perspectives for a vaccine against hepatitis C virus. J. Hepatol. 31 Suppl 1:259–63.
Hsu HH, Abrignani S, Houghton M. (1999) Prospects for a hepatitis C virus vaccine. Clin. Liver Dis. 3:901–15.
Liberman E, Fong YL, Selby MJ, Choo QL, Cousens L, Houghton M, Yen TS. (1999) Activation of the grp78 and grp94 promoters by hepatitis C virus E2 envelope protein. J. Virol. 73:3718–22.
Mustilli AC, Izzo E, Houghton M, Galeotti CL. (1999) Comparison of secretion of a hepatitis C virus glycoprotein in Saccharomyces cerevisiae and Kluyveromyces lactis. Res. Microbiol. 150:179–87.
Rosen HR, Hinrichs DJ, Gretch DR, Koziel MJ, Chou S, Houghton M, Rabkin J, Corless CL, Bouwer HG. (1999) Association of multispecific CD4(+) response to hepatitis C and severity of recurrence after liver transplantation. Gastroenterology. 117:926–32.
Allander T, Drakenberg K, Beyene A, Rosa D, Abrignani S, Houghton M, Widell A, Grillner L, Persson MA. (2000) Recombinant human monoclonal antibodies against different conformational epitopes of the E2 envelope glycoprotein of hepatitis C virus that inhibit its interaction with CD81. J. Gen. Virol. 81:2451–9.
Alter HJ, Houghton M. (2000) Clinical Medical Research Award. Hepatitis C virus and eliminating post-transfusion hepatitis. Nat. Med. 6:1082–6.
Fan XG, Tang FQ, Yi H, Liu WE, Houghton M, Hu GL. (2000) Effect of IL-12 on T-cell immune responses in patients with chronic HCV infection. APMIS. 108:531–8.
Heile JM, Fong YL, Rosa D, Berger K, Saletti G, Campagnoli S, Bensi G, Capo S, Coates S, Crawford K, Dong C, Wininger M, Baker G, Cousens L, Chien D, Ng P, Archangel P, Grandi G, Houghton M, Abrignani S. (2000) Evaluation of hepatitis C virus glycoprotein E2 for vaccine design: an endoplasmic reticulum-retained recombinant protein is superior to secreted recombinant protein and DNA-based vaccine candidates. J. Virol. 74:6885–92.
Houghton M. (2000) Strategies and prospects for vaccination against the hepatitis C viruses. Curr. Top. Microbiol. Immunol. 242:327–39. Review.
Lee AY, Manning WC, Arian CL, Polakos NK, Barajas JL, Ulmer JB, Houghton M, Paliard X. (2000) Priming of hepatitis C virus-specific cytotoxic T lymphocytes in mice following portal vein injection of a liver-specific plasmid DNA. Hepatology. 31:1327–33.
Lee AY, Polakos NK, Otten GR, Ulmer JB, Houghton M, Paliard X. (2000) Quantification of the number of cytotoxic T cells specific for an immunodominant HCV-specific CTL epitope primed by DNA immunization. Vaccine. 18:1962–8.
Petracca R, Falugi F, Galli G, Norais N, Rosa D, Campagnoli S, Burgio V, Di Stasio E, Giardina B, Houghton M, Abrignani S, Grandi G. (2000) Structure-function analysis of hepatitis C virus envelope-CD81 binding. J. Virol. 74:4824–30.
Weiner A, Chien D, Choo Q-L, Coates S, Kuo G, Houghton M. (2000) “Humoral response to HCV” in Hepatitis C. (Liang J, Hoofnagle J. eds.), pp. 125–145. Academic Press.
Schirren CA, Jung MC, Gerlach JT, Worzfeld T, Baretton G, Mamin M, Hubert Gruener N, Houghton M, Pape GR. (2000) Liver-derived hepatitis C virus (HCV)-specific CD4(+) T cells recognize multiple HCV epitopes and produce interferon gamma. Hepatology. 32:597–603.
Bassett SE, Guerra B, Brasky K, Miskovsky E, Houghton M, Klimpel GR, Lanford RE. (2001) Protective immune response to hepatitis C virus in chimpanzees rechallenged following clearance of primary infection. Hepatology. 33:1479–87.
Erickson AL, Kimura Y, Igarashi S, Eichelberger J, Houghton M, Sidney J, McKinney D, Sette A, Hughes AL, Walker CM. (2001) The outcome of hepatitis C virus infection is predicted by escape mutations in epitopes targeted by cytotoxic T lymphocytes. Immunity. 15:883–95.
Merola M, Brazzoli M, Cocchiarella F, Heile JM, Helenius A, Weiner AJ, Houghton M, Abrignani S. (2001) Folding of hepatitis C virus E1 glycoprotein in a cell-free system. J. Virol. 75:11205–17.
Polakos NK, Drane D, Cox J, Ng P, Selby MJ, Chien D, O’Hagan DT, Houghton M, Paliard X. (2001) Characterization of hepatitis C virus core-specific immune responses primed in rhesus macaques by a nonclassical ISCOM vaccine. J. Immunol. 166:3589–98.
Schirren CA, Jung MC, Worzfeld T, Mamin M, Baretton G, Gerlach JT, Gruener NH, Zachoval R, Houghton M, Rau HG, Pape GR. (2001) Hepatitis C virus-specific CD4+ T cell response after liver transplantation occurs early, is multispecific, compartmentalizes to the liver, and does not correlate with recurrent disease. J. Infect. Dis. 183:1187–94.
Tseng CT, Miskovsky E, Houghton M, Klimpel GR. (2001) Characterization of liver T-cell receptor gammadelta T cells obtained from individuals chronically infected with hepatitis C virus (HCV): evidence for these T cells playing a role in the liver pathology associated with HCV infections. Hepatology. 33:1312–20.
Weiner AJ, Paliard X, Selby MJ, Medina-Selby A, Coit D, Nguyen S, Kansopon J, Arian CL, Ng P, Tucker J, Lee CT, Polakos NK, Han J, Wong S, Lu HH, Rosenberg S, Brasky KM, Chien D, Kuo G, Houghton M. (2001) Intrahepatic genetic inoculation of hepatitis C virus RNA confers cross-protective immunity. J. Virol. 75:7142–8.
Legrand E, Neau D, Galperine T, Trimoulet P, Moreau JF, Pitard V, Lacut JY, Ragnaud JM, Dupon M, Le Bail B, Bernard N, Schvoerer E, Houghton M, Fleury H, Lafon ME. (2002) CD4 T lymphocyte proliferative responses to hepatitis C virus (HCV) antigens in patients coinfected with HCV and human immunodeficiency virus who responded to anti-HCV treatment. J. Infect. Dis. 186:302–11.
Masciopinto F, Freer G, Burgio VL, Levy S, Galli-Stampino L, Bendinelli M, Houghton M, Abrignani S, Uematsu Y. (2002) Expression of human CD81 in transgenic mice does not confer susceptibility to hepatitis C virus infection. Virology. 304:187–96.
Shoukry NH, Grakoui A, Houghton M, Chien DY, Ghrayeb J, Reimann KA, Walker CM. (2003) Memory CD8+ T cells are required for protection from persistent hepatitis C virus infection. J. Exp. Med. 197:1645–55.
Seo MY, Abrignani S, Houghton M, Han JH. (2003) Small interfering RNA-mediated inhibition of hepatitis C virus replication in the human hepatoma cell line Huh-7. J. Virol. 77:810–2.
Masciopinto F, Giovani C, Campagnoli S, Galli-Stampino L, Colombatto P, Brunetto M, Yen TS, Houghton M, Pileri P, Abrignani S. (2004) Association of hepatitis C virus envelope proteins with exosomes. Eur. J. Immunol. 34:2834–42.
Houghton M, Abrignani S. (2004) “Vaccination against the hepatitis C viruses” in New Generation Vaccines 3rd Edition (Levine MM, Kaper JB, Rappuoli R, Liu M, Good MF. eds.) pp. 593–606. Marcel Dekker Inc., New York.
O’Hagan DT, Singh M, Dong C, Ugozzoli M, Berger K, Glazer E, Selby M, Wininger M, Ng P, Crawford K, Paliard X, Coates S, Houghton M. (2004) Cationic microparticles are a potent delivery system for a HCV DNA vaccine. Vaccine. 23:672–80.
Coates S, Choo Q-L, Kuo G, Crawford K, Dong C, Wininger M, Weiner A, Abrignani S, Houghton M. (2004) “Hepatitis C” in Vaccines: Preventing Disease & Protecting Health (De Quadros CA. ed.) pp. 150–6. Pan American Health Organisation.
Song HC, Seo MY, Stadler K, Yoo BJ, Choo QL, Coates SR, Uematsu Y, Harada T, Greer CE, Polo JM, Pileri P, Eickmann M, Rappuoli R, Abrignani S, Houghton M, Han JH. (2004) Synthesis and characterization of a native, oligomeric form of recombinant severe acute respiratory syndrome coronavirus spike glycoprotein. J. Virol. 78:10328–35.
Brazzoli M, Helenius A, Foung SK, Houghton M, Abrignani S, Merola M. (2005) Folding and dimerization of hepatitis C virus E1 and E2 glycoproteins in stably transfected CHO cells. Virology. 332:438–53.
Coates S, Choo Q-L, Kuo G, Crawford K, Dong C, Wininger M, Weiner A, Berger K, Wong S, Ralston R, Morandi M, Pileri P, Rosa D, Muchmore E, Mahoney J, Brasky K, Purcell R, Abrignani S, Houghton, M. (2005) “Protection of chimpanzees against heterologous 1a viral challenge using a gpE1/gpE2 heterodimer vaccine” in Proceedings of the 11th International Symposium on Viral Hepatitis & Liver Disease (Jilbert AR, Grgacic EVL, Vickery K, Burrell CJ, Cossart YE. eds.) pp. 118–123. Australian Center for Hepatitis Virology.
Nattermann J, Schneiders AM, Leifeld L, Langhans B, Schulz M, Inchauspe G, Matz B, Brackmann HH, Houghton M, Sauerbruch T, Spengler U. (2005) Serum antibodies against the hepatitis C virus E2 protein mediate antibody-dependent cellular cytotoxicity (ADCC). J. Hepatol. 42:499–504.
Houghton M, Abrignani S. (2005) Prospects for a vaccine against the hepatitis C virus. Nature. 436:961–6.
Rosa D, Saletti G, De Gregorio E, Zorat F, Comar C, D’Oro U, Nuti S, Houghton M, Barnaba V, Pozzato G, Abrignani S. (2005) Activation of naive B lymphocytes via CD81, a pathogenic mechanism for hepatitis C virus-associated B lymphocyte disorders. Proc. Natl. Acad. Sci. USA. 102:18544–9.
Vajdy M, Selby M, Medina-Selby A, Coit D, Hall J, Tandeske L, Chien D, Hu C, Rosa D, Singh M, Kazzaz J, Nguyen S, Coates S, Ng P, Abrignani S, Lin Y-L, Houghton M, O’Hagan D. (2006) Hepatitis C virus polyprotein vaccine formulations capable of inducing broad antibody and cellular immune responses. J. Gen. Virol. 87:2253–62.
Stamataki Z, Coates S, Evans MJ, Wininger M, Crawford K, Dong C, Fong YL, Chien D, Abrignani S, Balfe P, Rice CM, McKeating JA, Houghton M. (2007) Hepatitis C virus envelope glycoprotein immunization of rodents elicits cross-reactive neutralizing antibodies. Vaccine. 25:7773–84.
Manns MP, Foster GR, Rockstroh JK, Zeuzem S, Zoulim F, Houghton M. (2007) The way forward in HCV treatment – finding the right path. Nat. Rev. Drug Discov. 6:991–1000. Review. Erratum in: Nat. Rev. Drug Discov. (2008) 7:102. Nat. Rev. Drug Discov. (2008) 7:458.
Bowen DG, Shoukry NH, Grakoui A, Fuller MJ, Cawthon AG, Dong C, Hasselschwert DL, Brasky KM, Freeman GJ, Seth NP, Wucherpfennig KW, Houghton M, Walker CM. (2008) Variable patterns of programmed death-1 expression on fully functional memory T cells after spontaneous resolution of hepatitis C virus infection. J. Virol. 82:5109–14.
Lin Y, Kwon T, Polo J, Zhu YF, Coates S, Crawford K, Dong C, Wininger M, Hall J, Selby M, Coit D, Medina-Selby A, McCoin C, Ng P, Drane D, Chien D, Han J, Vajdy M, Houghton M. (2008) Induction of broad CD4+ and CD8+ T-cell responses and cross-neutralizing antibodies against hepatitis C virus by vaccination with Th1-adjuvanted polypeptides followed by defective alphaviral particles expressing envelope glycoproteins gpE1 and gpE2 and nonstructural proteins 3, 4, and 5. J. Virol. 82:7492–503.
Houghton M. (2009) Discovery of the hepatitis C virus. Liver Int. 29 Suppl 1:82–8. Review.
Houghton M. (2009) The long and winding road to the identification of the hepatitis C virus. J. Hepatol. 51:939–48.
Drane D, Maraskovsky E, Gibson R, Mitchell S, Barnden M, Moskwa A, Shaw D, Gervase B, Coates S, Houghton M, Basser R. (2009) Priming of CD4+ and CD8+ T cell responses using a HCV core ISCOMATRIX vaccine: a phase I study in healthy volunteers. Hum. Vaccin. 5:151–7.
Ray R, Meyer K, Banerjee A, Basu A, Coates S, Abrignani S, Houghton M, Frey SE, Belshe RB. (2010) Characterization of antibodies induced by vaccination with hepatitis C virus envelope glycoproteins. J. Infect. Dis. 202:862–6.
Frey SE, Houghton M, Coates S, Abrignani S, Chien D, Rosa D, Pileri P, Ray R, Di Bisceglie AM, Rinella P, Hill H, Wolff MC, Schultze V, Han JH, Scharschmidt B, Belshe RB. (2010) Safety and immunogenicity of HCV E1E2 vaccine adjuvanted with MF59 administered to healthy adults. Vaccine. 28:6367–73.
Houghton M. (2011) Prospects for prophylactic and therapeutic vaccines against the hepatitis C viruses. Immunol. Rev. 239:99–108.
Stamataki Z, Coates S, Abrignani S, Houghton M, McKeating, J. (2011) Immunization of human volunteers with Hepatitis C virus envelope glycoproteins elicits antibodies that cross-neutralize heterologous virus strains. J. Infect. Dis. 204:811–3.
Meunier JC, Gottwein JM, Houghton M, Russell RS, Emerson SU, Bukh J, Purcell RH. (2011) Vaccine-induced cross-genotype reactive neutralizing antibodies against hepatitis C virus. J. Infect. Dis. 204:1186–90.
Houghton M. (2012) Chimp virus makes a savvy vaccine vector. Sci. Transl. Med. 4:115fs1.
Law JLM, Chen C, Wong J, Hockman D, Santer DM, Frey SE, Belshe RB, Wakita T, Bukh J, Jones CT, Rice CM, Abrignani S, Tyrrell DL, Houghton M. (2013) A hepatitis C virus (HCV) vaccine comprising envelope glycoproteins gpE1/ gpE2 derived from a single isolate elicits broad cross-genotype neutralizing antibodies in humans. PLoS ONE. 8:e59776. doi:10.1371/journal. pone.0059776.
Houghton M. (2013) Three isn’t the magic number. Nat. Med. 19:807.
Santer DM, Ma MM, Hockman D, Landi A, Tyrrell DL, Houghton M. (2013) Enhanced activation of memory, but not naïve, B cells in chronic hepatitis C virus-infected patients with cryoglobulinemia and advanced liver fibrosis. PLoS ONE. 8:e68308. doi: 10.1371/journal.pone.0068308.
Nourbakhsh M, Douglas DN, Pu CH, Lewis JT, Kawahara T, Lisboa LF, Wei E, Asthana S, Quiroga AD, Law LM, Chen C, Addison WR, Nelson R, Houghton M, Lehner R, Kneteman NM. (2013) Arylacetamide deacetylase: A novel host factor with important roles in the lipolysis of cellular triacylglycerol stores, VLDL assembly and HCV production. J. Hepatol. 59:336–43.
Houghton M, Law J, Tyrrell DL. (2013) An inactivated hepatitis C virus vaccine on the horizon? Gastroenterology. 145:285–8.
Grebely J, Bilodeau M, Feld JJ, Bruneau J, Fischer B, Raven JF, Roberts E, Choucha N, Myers RP, Sagan SM, Wilson JA, Bialystok F, Tyrrell DL, Houghton M, Krajden M. (2013) The Second Canadian Symposium on Hepatitis C Virus: A call to action. Can. J. Gastroenterol. 27:627–32.
Steenbergen RH, Joyce MA, Thomas BS, Jones D, Law J, Russell R, Houghton M, Tyrrell DL. (2013) Human serum leads to differentiation of human hepatoma cells, restoration of very-low-density lipoprotein secretion, and a 1000-fold increase in HCV Japanese fulminant hepatitis type 1 titers. Hepatology. 58:1907–17.
Law LMJ, Landi A, Magee WC, Tyrrell DL, Houghton M. (2013) Progress towards a hepatitis C virus vaccine. Emerg. Microbes Infect. 2:e79. doi:10.1038/emi.2013.79.
Colombatto P, Brunetto MR, Maina AM, Romagnoli V, Almasio P, Rumi MG, Ascione A, Pinzello G, Mondelli M, Muratori L, Rappuoli R, Rosa, D, Houghton M, Abrignani S, Bonino F. (2013) HCV E1E2-MF59 vaccine in chronic hepatitis C patients treated with PEG-IFNα2a and ribavirin: a randomized controlled trial. J. Viral Hepatitis. doi: 10.1111/jvh.12163.
Houghton M. (2014) Hepatitis C: the next 25 years. Antiviral Res.110:77–8. doi: 10.1016/j.antiviral.2014.06.018.
Wong JA, Bhat R, Hockman D, Logan M, Chen C, Levin A, Frey SE, Belshe RB, Tyrrell DL, Law JL, Houghton M. (2014) Recombinant hepatitis C virus envelope glycoprotein vaccine elicits antibodies targeting multiple epitopes on the envelope glycoproteins associated with broad cross-neutralization. J Virol. 88:14278–88. doi: 10.1128/JVI.01911-14.
MacParland SA, Bilodeau M, Grebely J, Bruneau J, Cooper C, Klein M, Sagan S, Choucha N, Balfour L, Bialystok F, Krajden M, Raven J, Roberts E, Russell R, Houghton M, Tyrrell DL, Feld JJ. (2014) National CIHR Research Training Program in Hepatitis C. The 3rd Canadian Symposium on Hepatitis C Virus: expanding care in the interferon-free era. Can J Gastroenterol Hepatol. 28:481–7.
Ahmed M, Wang F, Levin A, Le C, Eltayebi Y, Houghton M, Tyrrell L, Barakat K. (2015) Targeting the Achilles heel of the hepatitis B virus: a review of current treatments against covalently closed circular DNA. Drug Discov Today. 20:548–61. doi: 10.1016/j.drudis.2015.01.008.
Logan M, Law J, Wong JA, Hockman D, Landi A, Chen C, Crawford K, Kundu J, Baldwin L, Johnson J, Dahiya A, LaChance G, Marcotrigiano J, Law M, Foung S, Tyrrell L, Houghton M.(2016) Native folding of a recombinant gpe1/gpe2 heterodimer vaccine antigen from a precursor protein fused with Fc IgG. J Virol. 91:e01552-16 doi:10.1128/JVI.01552-16.
Huang W, Wang Y, Chen C, Law JL, Houghton M, Chen L. (2016) Fabrication of flexible self-standing all-cellulose nanofibrous composite membranes for virus removal. Carbohydrate Polymers. 143:9–17. doi: 10.1016/j.carbpol.2016.02.011.
O’Shea D, Law J, Egli A, Douglas D, Lund G, Forester S, Lambert J, Law M, Burton DR, Tyrrell DL, Houghton M, Humar A, Kneteman N. (2016) Prevention of hepatitis C virus infection using a broad cross-neutralizing monoclonal antibody (AR4A) and epigallocatechin gallate. Liver Transplantation. 22:324–32. doi: 10.1002/lt.24344.
Freedman H, Logan MR, Law JL, Houghton M. (2016) Structure and Function of the Hepatitis C Virus Envelope Glycoproteins E1 and E2: Antiviral and Vaccine Targets. ACS Infect Dis. 2:749–762. Epub 2016 Aug 16
Freedman H, Logan MR, Hockman D, Leman JK,, Law JL, Houghton M. (2017) Computational Prediction of the Heterodimeric and Higher Order Structure of gpE1/gpE2 Envelope Glycoproteins Encoded by the Hepatitis C Virus (HCV). J Virol. doi: 10.1128/JVI.02309-16.
Sarhan MA, Abdel-Hakeem MS, Mason AL, Tyrrell DL, Houghton M. (2017) Glycogen Synthase Kinase 3β Inhibitors Prevent Hepatitis C Virus Release/Assembly through Perturbation of Lipid Metabolism. Scientific Reports. doi: 10.1038/ s41598-017-02648-6
Landi A, Law J, Hockman D, Logan M, Crawford K, Chen C, Kundu J, Ebensen T, Guzman CA, Deschatelets L, Krishnan L, Tyrrell DLJ, Houghton M. (2017) Superior immunogenicity of HCV envelope glycoproteins when adjuvanted with cyclic-di-AMP, a STING activator or archaeosomes. Vaccine. 35:6949– 6956 doi: 10.1016/j.vaccine.2017.10.072.
Bartenschlager R, Baumert TF, Bukh J, Houghton M, Lemon SM, Lindenbach BD, Lohmann V, Moradpour D, Pietschmann T, Rice CM, Thimme R, Wakita T. (2018). Critical challenges and emerging opportunities in Hepatitis C virus research in an era of potent antiviral therapy: Considerations for scientists and funding agencies. Virus research. 248:53–62. doi: 10.1016/j.virusres.2018.02.016
Law JLM, Logan M, Wong J, Kundu J, Hockman D, Landi A, Chen C, Crawford K, Wininger M, Johnson J, Mesa Prince C, Dudek E, Mehta N, Tyrrell DL, Houghton M. (2018) Role of the E2 Hypervariable Region (HVR1) in the Immunogenicity of a Recombinant Hepatitis C Virus Vaccine. Journal of virology. 92. pii: e02141-17. doi: 10.1128/JVI.02141-17.
Khera T, Behrendt P, Bankwitz D, Brown RJP, Todt D, Doepke M, Khan AG, Schulze K, Law J, Logan M, Hockman D, Wong JAJ, Dold L, Gonzalez-Motos V, Spengler U, Viejo-Borbolla A, Ströh LJ, Krey T, Tarr AW, Steinmann E, Manns MP, Klein F, Guzman CA, Marcotrigiano J, Houghton M, Pietschmann T. (2018) Functional and immunogenic characterization of diverse HCV glycoprotein E2 variants. J Hepatol. doi: 10.1016/j.jhep.2018.11.003
Banda DH, Perin PM, Brown RJP, Todt D, Solodenko W, Hoffmeyer P, Kumar Sahu K, Houghton M, Meuleman P, Müller R, Kirschning A, Pietschmann T.(2019) A central hydrophobic E1 region controls the pH range of hepatitis C virus membrane fusion and susceptibility to fusion inhibitors. J Hepatol. 70(6):1082–1092. doi: 10.1016/j.jhep.2019.01.033. Epub 2019 Feb 13.
Houghton M. (2019) Hepatitis C Virus: 30 Years after Its Discovery. Cold Spring Harb Perspect Med. 9(12). doi: 10.1101/cshperspect.a037069.
Akache B, Deschatelets L, Harrison BA, Dudani R, Stark FC, Jia Y, Landi A, Law JLM, Logan M, Hockman D, Kundu J, Tyrrell DL, Krishnan L, Houghton M, McCluskie MJ. (2019) Effect of Different Adjuvants on the Longevity and Strength of Humoral and Cellular Immune Responses to the HCV Envelope Glycoproteins. Vaccines (Basel). 7(4). doi: 10.3390/vaccines7040204.
Immunoregulation
Egli A, Levin A, Santer DM, Joyce M, O’Shea D, Thomas BS, Lisboa LF, Barakat K, Bhat R, Fischer KP, Houghton M, Tyrrell DL, Kumar D, Humar A. (2014) Immunomodulatory Function of Interleukin 28B during primary infection with cytomegalovirus. J Infect Dis. 210:717–27. doi: 10.1093/infdis/jiu144.
Egli A, Santer D, Barakat K, Zand M, Levin A, Vollmer M, Weisser M, Khanna N, Kumar D, Tyrrell L, Houghton M, Battegay M, O’Shea D. (2014) Vaccine adjuvants-understanding molecular mechanisms to improve vaccines. Swiss Med Wkly. 144:w13940. doi: 10.4414/smw.2014.13940. eCollection 2014.
Egli A, Santer DM, O’Shea D, Barakat K, Syedbasha M, Vollmer M, Baluch A, Bhat R, Groenendyk J, Joyce MA, Lisboa LF, Thomas BS, Battegay M, Khanna N, Mueller T, Tyrrell DL, Houghton M, Humar A, Kumar D. (2014) IL-28B is a key regulator of B-and T-cell vaccine responses against influenza. PLoS Pathog. 10:e1004556. doi: 10.1371/journal.ppat.1004556. eCollection 2014 Dec.
Egli A, Santer DM, O’Shea D, Tyrrell DL, Houghton M. (2014) The impact of the interferon-lambda family on the innate and adaptive immune response to viral infections. Emerging Microbes Infections. 3:e51. doi: 10.1038/emi.2014.51.
Egli A, Humar A, Widmer LA, Lisboa LF, Santer DM, Mueller T, Stelling J, Baluch A, O’Shea D, Houghton M, Kumar D. (2015) Effect of Immunosuppression on T-Helper 2 and B-Cell Responses to Influenza Vaccination. J Infect Dis. 212:137–46. doi: 10.1093/infdis/jiv015.
Syedbasha M, Linnik J, Santer D, O’Shea D, Barakat K, Joyce M, Khanna N, Tyrrell DL, Houghton M, Egli A. (2016) An ELISA Based Binding and Competition Method to Rapidly Determine Ligand-receptor Interactions. J Vis Exp. doi: 10.3791/53575.
Santer DM, Minty GE, Mohamed A, Baldwin L, Bhat R, Joyce M, Egli A, Tyrrell DL, Houghton M. (2017) A novel method for detection of IFN-lambda 3 binding to cells for quantifying IFN-lambda receptor expression. J Immunol Methods. doi:10.1016/j.jim.2017.03.001.
Okoye IS, Houghton M, Tyrrell L, Barakat K, Elahi S. (2017) Coinhibitory Receptor Expression and Immune Checkpoint Blockade: Maintaining a Balance in CD8+ T Cell Responses to Chronic Viral Infections and Cancer. Front Immunol. doi: 10.3389/fimmu.2017.01215. eCollection 2017.
Santer DM, Minty GES, Golec DP, Lu J, May J, Namdar A, Shah J, Elahi S, Proud D, Joyce M, Tyrrell DL, Houghton M. (2020) Differential expression of interferon-lambda receptor 1 splice variants determines the magnitude of the antiviral response induced by interferon-lambda 3 in human immune cells. PLoS Pathog. 16(4):e1008515. doi: 10.1371/journal.ppat.1008515
Freedman H, Kundu J, Tchesnokov EP, Law JLM, Nieman JA, Schinazi RF, Tyrrell DL, Gotte M, Houghton M. (2020) Application of Molecular Dynamics Simulations to the Design of Nucleotide Inhibitors Binding to Norovirus Polymerase. J Chem Inf Model. 60(12):6566–6578. doi: 10.1021/acs.jcim.0c00742. Epub 2020 Dec 1. PMID: 33259199; PMCID: PMC7869559.
Autoimmune Liver Disease
Landi A, Weismuller TJ, Lankisch TO, Santer DM, Tyrrell DL, Manns MP, Houghton M. (2014) Differential serum levels of eosinophilic eotaxins in primary sclerosing cholangitis, primary biliary cirrhosis, and autoimmune hepatitis. J Interferon Cytokine Res. 34(3):204–14. doi: 10.1089/jir.2013.0075.
Chronic Fatigue Syndrome
Steffen I, Tyrrell DL, Stein E, Montalvo L, Lee TH, Zhou Y, Lu K, Switzer WM, Tang S, Jia H, Hockman D, Santer DM, Logan M, Landi A, Law J, Houghton M, Simmons G. (2011) No evidence for XMRV nucleic acids, infectious virus or anti-XMRV antibodies in Canadian patients with chronic fatigue syndrome. PLoS ONE. 6:e27870.
Jason LA, Unger ER, Dimitrakoff JD, Fagin AP, Houghton M, Cook DB, Marshall GD Jr, Klimas N, Snell C. (2012) Minimum data elements for research reports on CFS. Brain Behav. Immun. 26:401–6.
Landi A, Broadhurst D, Vernon SD, Tyrrell DL, Houghton M. (2015) Reductions in circulating levels of IL-16, IL-7 and VEGF-A in myalgic encephalomyelitis/ chronic fatigue syndrome. Cytokine. 78:27–36. doi: 10.1016/j.cyto.2015.11.018.
Gindin Y, Chung C, Jiang Z, Zhou JZ, Xu J, Billin AN, Myers RP, Goodman Z, Landi A, Houghton M, Green RM, Levy C, Kowdley KV, Bowlus CL, Muir AJ, Trauner M. (2021) A Fibrosis-Independent Hepatic Transcriptomic Signature Identifies Drivers of Disease Progression in Primary Sclerosing Cholangitis. Hepatology. 73(3):1105–1116. doi: 10.1002/hep.31488. Epub 2021 Feb 28. PMID: 32745270; PMCID: PMC8048608.
Computational Modeling
Barakat KH, Huzil JT, Jordan KE, Evangelinos C, Houghton M, Tuszynski J. (2013) A computational model for overcoming drug resistance using selective dual-inhibitors for aurora kinase A and its T217D variant. Mol. Pharm. 10:4572–89.
Barakat KH, Law J, Prunotto A, Magee WC, Evans DH, Tyrrell DL, Tuszynski J, Houghton M. (2013) Detailed computational study of the active site of the hepatitis C viral RNA polymerase to aid novel drug design. J. Chem. Inf. Model. 53:3031–43.
Anwar-Mohamed A, Barakat KH, Bhat R, Noskov SY, Tyrrell DL, Tuszynski JA,Houghton M. (2014) A human ether-á-go-go-related (hERG) ion channel atomistic model generated by long supercomputer molecular dynamics simulations and its use in predicting drug cardiotoxicity. Toxicology Letters. 230:382–92. doi: 10.1016/j.toxlet.2014.08.007.
Barakat KH, Anwar-Mohamed A, Tuszynski JA, Robins MJ, Tyrrell DL, Houghton M. (2015) A Refined Model of the HCV NS5A protein bound to daclatasvir explains drug-resistant mutations and activity against divergent genotypes. J Chem Inf Model. 55:362–73. doi: 10.1021/ci400631n.
Ahmed M, Pal A, Houghton M, Barakat K. (2016) A Comprehensive Computational Analysis for the Binding Modes of Hepatitis C Virus NS5A Inhibitors: The Question of Symmetry. ACS Infect Dis. 2:872–881.
Ahmed M, Jalily Hasani H, Ganesan A, Houghton M, Barakat K. (2017) Modeling the human Nav1.5 sodium channel: structural and mechanistic insights of ion permeation and drug blockade. Drug Des Devel Ther. doi: 10.2147/DDDT. S133944. eCollection 2017.
Barakat KH, Houghton M, Tyrrell DL, Tuszynski JA. (2017) Rational Drug Design Rational Drug Design: One Target, Many Paths to It. IGI Global. doi: 10.4018/978-1-5225-1762-7.ch044
Freedman H, Winter P, Tuszynski J, Tyrrell DL, Houghton M. (2018) A computational approach for predicting off-target toxicity of antiviral ribonucleoside analogues to mitochondrial RNA polymerase. The Journal of biological chemistry. 293:9696–9705. doi: 10.1074/jbc.RA118.002588
Ganesan A, Ahmed M, Okoye I, Arutyunova E, Babu D, Turnbull W, Kundu JK, Shields J, Agopsowicz K, Xu L, Tabana Y, Srivastava N, Zhang G, Moon T, Belovodskiy A, Hena M, Kandadai AS, Hosseini S, Hitt M, Walker J, Smylie M, West FG, Siraki AG, Lemieux MJ, Elahi S, Nieman JA, Tyrrell DL, Houghton M, Barakat K. (2019) Comprehensive in vitro characterization of PD-L1 small molecule inhibitors. Scientific Reports. 9(1):12392. doi: 10.1038/s41598-019-48826-6.
Kalyaanamoorthy S, Lamothe SM, Hou X, Moon TC, Kurata HT, Houghton M, Barakat KH. (2020) A structure-based computational workflow to predict liability and binding modes of small molecules to hERG. Sci Rep. 10(1):16262. doi: 10.1038/s41598-020-72889-5.
Freedman H, Kundu J, Tchesnokov EP, Law JLM, Nieman JA, Schinazi RF, Tyrrell DL, Gotte M, Houghton M. (2020) Application of Molecular Dynamics Simulations to the Design of Nucleotide Inhibitors Binding to Norovirus Polymerase. J Chem Inf Model.; 60(12):6566–6578. doi: 10.1021/acs.jcim.0c00742.
COVID-19
Law JLM, Logan M, Joyce MA, Landi A, Hockman D, Crawford K, Johnson J, LaChance G, Saffran HA, Shields J, Hobart E, Brassard R, Arutyunova E, Pabbaraju K, Croxen M, Tipples G, Lemieux MJ, Tyrrell DL, Houghton M. (2021) SARS-COV-2 recombinant Receptor-Binding-Domain (RBD) induces neutralizing antibodies against variant strains of SARS-CoV-2 and SARS-CoV-1. Vaccine. 39(40):5769–5779. doi: 10.1016/j.vaccine.2021.08.081. Epub 2021 Aug 26. PMID: 34481699; PMCID: PMC8387217.
Photo of Michael Houghton © University of Alberta
© The Nobel Foundation 2024
FAQ – Frequently asked questions
Do you have questions about the Nobel Prize and the Nobel Prize laureates? You’re in the right place. Keep scrolling down to find answers to our most commonly asked questions.
The Nobel Prize
- Why is there a Nobel Prize?
- Who was Alfred Nobel?
- How long have you been awarding the Nobel Prizes?
- What are the Nobel Prize categories?
- Why isn’t there a Nobel Prize in mathematics, engineering, biology or environmental science?
- Why is the Nobel Peace Prize awarded in Norway?
- Where does the prize money come from?
- Is it possible to revoke a Nobel Prize?
Nobel Prize laureates
- Why are they called Nobel Prize laureates?
- How many people can share the same Nobel Prize?
- Can you award a prize posthumously?
- Can someone affiliated with an organisation (like the EU or the IPCC) which was awarded the Nobel Peace Prize claim to have received the honour?
- How do you look upon criticism of Nobel Peace Prize laureates after they have been awarded?
- How can I contact a Nobel Prize laureate?
How Nobel Prize laureates are chosen
- Who selects the Nobel Prize laureates?
- How do you become nominated?
- How do you become a nominator?
- Is being nominated an endorsement by the Nobel Prize?
- Are three nominations enough to be awarded the Nobel Prize?
- Is it possible to nominate someone for a posthumous Nobel Prize?
- Can I find out who has been nominated for a Nobel Prize?
- Can an eligible nominator reveal who they have nominated for the Nobel Prize within 50 years?
- How do the committees decide who to award the prizes to?
- Is it possible for a committee to look over my work?
- Do the Nobel Committees ever reconsider a choice?
- What if the awarded inventions fail after some time, say two years later?
The Nobel Prize award ceremonies
The Nobel Prize
Why is there a Nobel Prize?
The Nobel Prize was set up when businessman and entrepreneur Alfred Nobel died and left the majority of his fortune to the establishment of prizes in physics, chemistry, physiology or medicine, literature and peace. His will stated that the prizes should be awarded to “those who, during the preceding year, shall have conferred the greatest benefit to humankind.”
Find out more about the establishment of the Nobel Prizes
Who was Alfred Nobel?
Alfred Nobel was an inventor, entrepreneur, scientist and businessman who also wrote poetry and drama. His varied interests are reflected in the Nobel Prizes which he laid the foundation for in 1895 in his last will and testament.
Learn more about Alfred Nobel
How long have you been awarding Nobel Prizes?
The first Nobel Prizes were awarded in 1901 and they have been awarded annually since then. There have been years in that time when the Nobel Prizes have not been awarded - mostly during World War I (1914–1918) and II (1939–1945).
See a full list of all Nobel Prizes
What are the Nobel Prize categories?
The Nobel Prize categories are physics, chemistry, physiology or medicine, literature and peace – these were laid out in the will of Alfred Nobel. In 1968, Sveriges Riksbank (Sweden’s central bank) established the Sveriges Riksbank Prize in Economic Sciences in Memory of Alfred Nobel.
Why isn’t there a Nobel Prize in mathematics, engineering, biology or environmental science?
The Nobel Prizes were designated in the will of Alfred Nobel and are in physics, chemistry, physiology or medicine, literature and peace. The economics prize was established much later and is a memorial prize, as indicated by its full name: the Sveriges Riksbank Prize in Economic Sciences in Memory of Alfred Nobel. Its addition was an exception, to celebrate the tercentenary of Sweden’s central bank in 1968.
Why is the Nobel Peace Prize awarded in Norway?
In his will Alfred Nobel laid out who he wanted to be responsible for the selection of the Nobel Prize laureates. The prizes were to be awarded by Swedish institutions – apart from the peace prize, whose award was to be decided by a committee of five persons elected by the Norwegian Parliament.
During Nobel’s lifetime Sweden and Norway were joined in a union but we still don’t know exactly why Alfred Nobel chose for the peace prize to be awarded in Norway. However as the prize committee is located in Oslo, it follows that the prize is also awarded there.
More about the Norwegian Nobel committee
Where does the prize money come from?
When Alfred Nobel died leaving the majority of his fortune to the establishment of the Nobel Prize he stated that the money should be converted into a fund and invested in “safe securities.” Today the interest earned on that money is used to fund the Nobel Prizes.
More about the prize money
Is it possible to revoke a Nobel Prize?
No. Neither Alfred Nobel’s will nor the statutes of the Nobel Foundation mention any such possibility.
Read a Q&A with Olav Njølstad, Director of the Norwegian Nobel Institute on this topic
Nobel Prize laureates
Why are they called Nobel Prize laureates?
The word “laureate” refers to being signified by the laurel wreath. In ancient Greece, laurel wreaths were awarded to victors as a sign of honour. Put that together with the Nobel Prize and we get “Nobel Prize laureate”.
More Nobel Prize facts
How many people can share the same Nobel Prize?
A Nobel Prize can be shared by up to three individuals, or in the case of the peace prize, it can also be awarded to an organisation. The rule that a prize can only be awarded to three people comes from the statutes of the Nobel Foundation, which is responsible for fulfilling the intentions of Nobel’s will. It specifically states: “In no case may a prize amount be divided between more than three persons.”
Read the statutes of the Nobel Foundation
Can you award a prize posthumously?
No, a Nobel Prize cannot be awarded posthumously.
However, since 1974, if the recipient dies after the prize has been announced they can still be awarded it. Previously, a person could be awarded a prize posthumously if they had already been nominated before 1 February of the same year, which was true of Erik Axel Karlfeldt (Nobel Prize in Literature 1931) and Dag Hammarskjöld (Nobel Peace Prize, 1961).
Following the 2011 announcement of the Nobel Prize in Physiology or Medicine, it was discovered that one of the medicine laureates, Ralph Steinman, had passed away three days earlier. The Board of the Nobel Foundation examined the statutes, and came to the conclusion that Ralph Steinman should continue to remain a Nobel Prize laureate, as the Nobel Assembly at Karolinska Institutet had announced the 2011 Nobel Prize laureates in physiology or medicine without knowing of his death.
Read the statutes of the Nobel Foundation
Can someone affiliated with an organisation (like the EU or the IPCC) which was awarded the Nobel Peace Prize claim to have received the honour?
When an organisation is awarded the Nobel Peace Prize the organisation becomes the laureate, not the individuals working there. Therefore those people connected to or working for a Nobel Prize awarded organisation cannot in any way refer to themselves personally as a Nobel Prize laureate.
How do you look upon criticism of Nobel Peace Prize laureates after they have been awarded?
For answers to this and other questions about the Nobel Peace Prize read a Q&A with Olav Njølstad, Director of the Norwegian Nobel Institute
How can I contact a Nobel Prize laureate?
The Nobel Foundation does not disclose addresses to Nobel Prize laureates out of courtesy. Please contact the institution, organisation or university to which the Nobel Prize laureate was affiliated at the time of the award. For literature laureates please contact their publishing house. Alternatively you may be able to contact some laureates via social media.
How Nobel Prize laureates are chosen
Who selects the Nobel Prize laureates?
In his last will and testament, Alfred Nobel specifically designated the institutions responsible for the prizes he wished to be established.
- The Royal Swedish Academy of Sciences for the Nobel Prize in Physics and Chemistry
- Karolinska Institutet (now The Nobel Assembly at Karolinska Institutet) for the Nobel Prize in Physiology or Medicine
- The Swedish Academy for the Nobel Prize in Literature
- A committee of five persons to be elected by the Norwegian Parliament (Storting) for the Nobel Peace Prize.
The Sveriges Riksbank Prize in Economic Sciences in Memory of Alfred Nobel was instituted in 1968, on the tercentenary of the bank. The Royal Swedish Academy of Sciences was given the task of selecting the economic sciences laureates. It has been awarded since 1969 according to the same principles as the Nobel Prizes.
Links to the prize-awarding institutions’ websites
How do you become nominated for a Nobel Prize?
In order to become a Nobel Prize laureate you must first be nominated for a prize by an eligible nominator. Self-nomination is not allowed. Except for the Nobel Peace Prize, nomination is by invitation only and nominators must fulfil the criteria set out by the awarding institutions.
Eligible nominations are then considered by the prize awarders, who make the final decision as to who will receive a Nobel Prize.
To find out who can be a nominator in each prize category, see the links below.
- Nomination and selection of physics laureates
- Nomination and selection of chemistry laureates
- Nomination and selection of medicine laureates
- Nomination and selection of literature laureates
- Nomination and selection of peace prize laureates
- Nomination and selection of economic sciences laureates
How can you become a nominator?
Only people who fulfil the criteria set out by the prize awarding institutions are allowed to nominate candidates for the Nobel Prize. To find out who can be a nominator in each prize category, see the links below.
- Nomination and selection of physics laureates
- Nomination and selection of chemistry laureates
- Nomination and selection of medicine laureates
- Nomination and selection of literature laureates
- Nomination and selection of peace laureates
- Nomination and selection of economic sciences laureates
Is being nominated an endorsement by the Nobel Prize?
No. Hundreds or thousands of nominations are received for the Nobel Prize every year from members of academies, university professors, scientists, previous Nobel Prize laureates, members of parliamentary assemblies and more.
In theory anybody could be put forward for a prize and as such being nominated is in no way an endorsement by the Nobel Prize. That is reserved for those individuals and organisations that are selected as Nobel Prize laureates.
Are three nominations enough to be awarded the Nobel Prize?
Frederick G. Banting and John Macleod were awarded the 1923 Nobel Prize in Physiology or Medicine the first year they were nominated (with three nominations) for their discovery of insulin. By contrast, Robert Koch was nominated 55 times over 4 years before he received the prize in 1905 for his discoveries concerning tuberculosis.
Search in the nomination archive for more information
Is it possible to nominate someone for a posthumous Nobel Prize?
No, it is not possible to nominate someone for a posthumous Nobel Prize.
See Can you award a prize posthumously? as well as paragraph 4 of the statutes of the Nobel Foundation.
Can I find out who has been nominated for a Nobel Prize?
Nominations can only be made public at least 50 years after the nomination has taken place – so nominations for this year’s Nobel Prizes are a closely guarded secret. Any rumours regarding recent nominees are either just rumour, or someone among the invited nominators has leaked information. Since the nominations are kept secret for at least 50 years, you’ll have to wait until then to find out.
For prizes older than 50 years old, you can browse the nomination archive. Note that in some cases the archives are sealed as long as people mentioned are still alive.
Can an eligible nominator reveal who they have nominated for the Nobel Prize within 50 years?
According to the statutes of the Nobel Foundation, information about the nominations is not to be disclosed, publicly or privately, for a period of fifty years. The restriction not only concerns the nominees and nominators, but also investigations and opinions in the awarding of a prize.
How do the committees decide who to award the prizes to?
Every committee is slightly different but ultimately they all work to fulfil the will of Alfred Nobel which stated that the Nobel Prize should be awarded according to those who have “conferred the greatest benefit to humankind.”
You can find out more about the process of selection for each Nobel Prize at the links below:
- Nomination and selection of physics laureates
- Nomination and selection of chemistry laureates
- Nomination and selection of medicine laureates
- Nomination and selection of literature laureates
- Nomination and selection of peace laureates
- Nomination and selection of economic sciences laureates
Is it possible for a committee to look over my work?
No, the committees cannot comment on work outside of their Nobel Prize responsibilities. It is not in the purpose of these committees to generally assess or evaluate any scientific or literary work beyond the assessment of nominations for the Nobel Prizes.
See also How do you become nominated for a Nobel Prize?
Do the Nobel Committees ever reconsider a choice?
No. For the very same reasons a prize cannot be revoked. According to the statutes of the Nobel Foundation, § 10, “No appeals may be made against the decision of a prize-awarding body with regard to the award of a prize”.
What if the awarded inventions fail after some time, say two years later?
A Nobel Prize cannot be revoked.
See also Do the Nobel Committees ever reconsider a choice?
The Nobel Prize award ceremonies
What is the Nobel Day?
The Nobel Day – which takes place on 10 December every year – marks the anniversary of Alfred Nobel’s death and is the day that the Nobel Prizes are presented to Nobel Prize laureates.
See Nobel Prize award ceremonies for more information.
Contact and copyright
Contact information for Nobel Prize-awarding institutions
For the Nobel Prizes in Physics and Chemistry and the Prize in Economic Sciences:
The Royal Swedish Academy of Sciences, see www.kva.se/en/contact-us/
For the Nobel Prize in Physiology or Medicine:
The Nobel Assembly at Karolinska Institutet, e-mail: [email protected]
For the Nobel Prize in Literature:
The Swedish Academy, e-mail: [email protected]
For the Nobel Peace Prize:
The Norwegian Nobel Committee, e-mail: [email protected]
Copyright photos and images
Can I use a photo of a Nobel Prize laureate?
For uses of photos permission from the Nobel Foundation or Nobel Prize Outreach AB, and in certain cases, from the photographer, is required. Read more: Copyright information
If permission is granted, “© The Nobel Foundation” or “© Nobel Prize Outreach” must be indicated.
The Nobel Foundation can unfortunately not grant permissions to use portrait photos of the Nobel Prize laureates of 1901–2006 due to copyright restrictions. We refer you to a photo agency such as sciencephoto.com, Scanpix, Reuters, Associated Press, Getty Images or Agence France Presse to make your enquiry for other photos. Where applicable, the university or institution to which the laureates were affiliated at the time of the award may be of assistance in providing photos. Please find information regarding such affiliations in the biographical information of each Nobel Prize laureate.
Starting in 2007, most of the official Nobel portraits on nobelprize.org are taken in Stockholm, with full copyright held by the Nobel Foundation. Please contact us if you wish to inquire about editorial use of these photos.
Can I use a photo from the Nobel Prize award ceremonies or Nobel Prize banquet?
The Nobel Foundation has only recently in cooperation with Nobel Prize Outreach begun making some images from the most recent ceremonies available for non-commercial, press and editorial use in the press room. Other photos from the Nobel Prize award ceremonies and banquets are published on nobelprize.org only. We refer external parties to contact photo agencies such as or sciencephoto.com, Scanpix, Reuters, Associated Press, Getty Images or Agence France Presse to make enquiries for other photos.
For more information please contact Nobel Prize Outreach.
Can I use a photo of a Nobel Prize medal?
No, you have to ask for permission from Nobel Prize Outreach.
I would like to request permission to use the Nobel name, the Nobel Prize medals and/or Nobel Prize insignias.
The Nobel Foundation is most restrictive in permitting the use of these trademarks. For details, see copyright information.
Can I use or translate a Nobel Prize lecture, speech or a biography?
Nobel Prize Outreach administrates the publishing rights of the Nobel Prize lectures, speeches and biographies on nobelprize.org on behalf of the Nobel Foundation who hold copyright. For information on how to license these, please see Copyright information/lectures.
To licence videos or texts, please see Copyright information/footage
Can I use an article?
No, you have to ask for permission from Nobel Prize Outreach. Please see Copyright information/articles
Can I use the material in press releases?
Yes, you can use texts and graphics from the press releases, whereas the use of logotypes and Nobel Prize design marks are not permitted. On all publications in full or in major parts the copyright notice must be applied as well as the source, https://www.nobelprize.org/. Read more: Copyright information/press releases
For press releases on the Nobel Prize in Physics, Chemistry and the Sveriges Riksbank Prize in Economic Sciences in Memory of Alfred Nobel: © The Royal Swedish Academy of Sciences
For press releases on the Nobel Prize in Physiology or Medicine: © The Nobel Assembly at Karolinska Institutet
For press releases on the Nobel Prize in Literature: © The Swedish Academy
For press releases on the Nobel Peace Prize: © The Norwegian Nobel Committee
Can I use text and pictures from scientific backgrounds, popular information and advanced information for the Nobel Prizes in Physics, Chemistry and the Sveriges Riksbank Prize in Economic Sciences in Memory of Alfred Nobel?
Yes, you can use texts and graphics from these documents for educational and editorial content intended for non-commercial purposes (use of logotypes and Nobel Prize design marks are not permitted). If the publications are used in its full version or excerpts are selected, the copyright notice must be applied, © The Royal Swedish Academy of Sciences, as well as the source, http://www.nobelprize.org/.
If you want to publish texts and graphics from these documents in a paper, journal or book, you have to ask for permission from the Royal Swedish Academy of Sciences, contact: [email protected].